AcceleDent does not reduce orthodontic pain: Another trial…..
AcceleDent does not reduce orthodontic pain: Another trial..
One of the main purposes of my blog is to help keep up with the literature and at the moment there are several papers being published on the clinical effects of methods of speeding up orthodontic treatment. Several manufacturers also claim that their innovations reduce orthodontic pain, as well as speed up tooth movement. This is a paper on whether AcceleDent reduces pain during orthodontic treatment.
Several months ago I posted on an interesting study in which the authors concluded that AcceleDent reduces orthodontic pain. In my post I pointed out that this was difficult to conclude from the paper because they did not use a placebo, which is necessary in pain studies. This new study addresses this issue.

Woodhouse, Neil R et al
Nature Scientific Report: 2015:5: 177224
DOI: 10.1038/srep17224
This paper was published in the high impact factor journal, Nature Scientific Reports. This is an open access journal. There appears to be a tendency for authors to publish in this type of journal rather than orthodontic journals. This is certainly good practice in terms of making information available, but it means that we need to be more effective when we search for journal papers. I hope that this blog can help!
This paper is a follow on report on results from a large study on the effectiveness of AcceleDent. I have already covered the paper on rate of initial alignment.
What did they do?
This was a three arm randomised trial in which participants were randomly allocated to:
- Orthodontic treatment as usual
- Orthodontic treatment plus AcceleDent (vibration)
- Orthodontic treatment plus sham AcceleDent (no vibration)
They gave the participants a Visual Analogue Scale (VAS) pain questionnaire to complete over the week following placement of the fixed appliance and insertion of the initial 0.014-inch nickel-titanium archwire (T1); and following insertion of a 0.018-inch nickel-titanium archwire (T2).They used the questionnaires to record pain when This was when the wires were fitted and then 4 hours, 24 hours, 3 days and 7 days later.
They also recorded initial tooth alignment and the use of oral analgesics.
They based their sample size calculation on the rate of alignment. Which is not the outcome being recorded in this study. As a result, there is a chance that the study could be underpowered to detect a difference. The authors went some way to address this by carrying out a further power calculation. This showed that the study had a power of greater than 80%, which is sufficient.
The randomisation, concealment and blinding were good. The statistical analysis was appropriate.
What did they find?
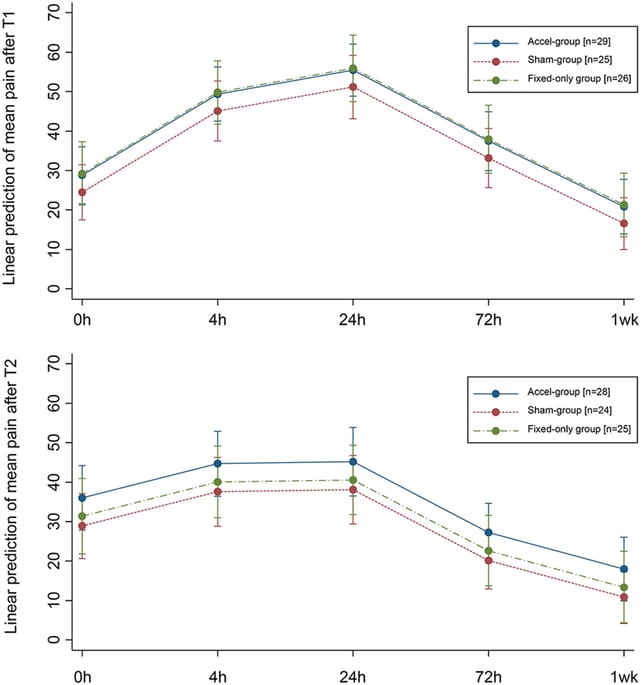
They found that there was no clinical or statistically significant effect of AcceleDent. Importantly, this was not influenced by whether the participants took oral analgesics.
The multivariate analysis showed that the only predictor of pain was time. Pain reduced with time. This is nicely shown in these graphs.
What did I think?
I have mentioned before that this is a good trial which is reported well. My only real concern was their decision to power their study on initial alignment, but they addressed this after the study.
The main strength of this study is that they used an inactive AcceleDent device as a placebo. Nevertheless, this may have had a biteplane effect and reduced pain. Importantly, there was also a further control of “no device” and again they did not detect any difference in pain. As a result, this paper is more scientifically sound than the previous paper (Lobre et al) , as a placebo effect was taken into account.
The authors also pointed out by the authors that they did not have accurate data on compliance, because the timers built into AcceleDent did not work. I have heard AcceleDent advocates raise this as a problem with this study. I disagree with this suggestion because the aim of the study is to evaluate of giving an intervention (AcceleDent). It is not compulsory to use the appliance, as a result, this adds a “real world” effect to the study. It is also relevant to point out the Lobre et al study, did not evaluate compliance.
I agree totally with the authors conclusions and I have repeated them here.
“This study has indicated that supplemental vibrational force provides no added value during initial tooth alignment with fixed appliances in terms of reducing the pain associated with this process. Given that this device is unlikely to be reimbursed in most countries, orthodontists should carefully consider their advice to orthodontic patients considering the use of AcceleDent as a method of pain relief. Current evidence would suggest that in appropriate patients, conventional non-prescription analgesia should be recommended if pain relief is required, with the caveat that pain is likely to reduce after the first 24 hours following archwire ligation and that in general, pain will be insignificant after a week”.
![]() Woodhouse, N., DiBiase, A., Papageorgiou, S., Johnson, N., Slipper, C., Grant, J., Alsaleh, M., & Cobourne, M. (2015). Supplemental vibrational force does not reduce pain experience during initial alignment with fixed orthodontic appliances: a multicenter randomized clinical trial Scientific Reports, 5 DOI: 10.1038/srep17224
Woodhouse, N., DiBiase, A., Papageorgiou, S., Johnson, N., Slipper, C., Grant, J., Alsaleh, M., & Cobourne, M. (2015). Supplemental vibrational force does not reduce pain experience during initial alignment with fixed orthodontic appliances: a multicenter randomized clinical trial Scientific Reports, 5 DOI: 10.1038/srep17224

Emeritus Professor of Orthodontics, University of Manchester, UK.
In 2012 we published the results of a study, which found that chewing gum reduced the impact and pain from fixed orthodontic appliances, without causing more breakages (Benson PE, et al. The effect of chewing gum on the impact, pain and breakages associated with fixed orthodontic appliances: a randomized clinical trial. Orthod Craniofac Res 2012; 15: 178-187). We received a few comments from participants that it didn’t actually reduce the pain, but acted as a distraction, which they found quite helpful.
The Visual Analogue Scale is a much-used tool to assess pain in orthodontic research, but I think the data are quite variable. A validated pain scale was developed in 2013 (Iwasaki, et al. Validation of a modified McGill Pain Questionnaire for orthodontic patients. Angle Orthod. 2013;83:906–912) and I would urge people to try it in future.