Early Class II treatment: Part 1: The wheel keeps turning. Uncertainty and the Pyramid of Denial
Early Class II treatment. The wheel keeps turning: Uncertainty and the Pyramid of Denial
This post is about early Class II treatment. I have decided to revisit this following a joint presentation that Jonathan Sandler and I did at the recent AAO congress in San Francisco.
 We were asked to participate in a point/counterpoint debate on early Class II treatment. Our role was to provide a counterpoint view to Drs Steven Dugoni and HeeSoo Oh from the University of the Pacific, Arthur Dugoni School of Dentistry, San Francisco. They have recently been promoting the benefits of early orthodontic treatment and run the early treatment clinic at the School.
We were asked to participate in a point/counterpoint debate on early Class II treatment. Our role was to provide a counterpoint view to Drs Steven Dugoni and HeeSoo Oh from the University of the Pacific, Arthur Dugoni School of Dentistry, San Francisco. They have recently been promoting the benefits of early orthodontic treatment and run the early treatment clinic at the School.
They started the debate by presenting the records of some selected well treated cases and the results of an unpublished retrospective study based on patient records selected from a convenience sample. They also suggested that the results of the three well-known randomised trials into early treatment were not valid because of a lack of generality and the patients were not retained between the phase 1 and phase 2 components of their treatment.
 Jonathan started the counterpoint view by summarising the current state of research knowledge based on the randomised trials and systematic reviews. (I have covered this in these posts). He also discussed important clinical aspects of early treatment and emphasised that most patients cannot wear retainers for the 2 to 3 years between phase 1 and phase 2.
Jonathan started the counterpoint view by summarising the current state of research knowledge based on the randomised trials and systematic reviews. (I have covered this in these posts). He also discussed important clinical aspects of early treatment and emphasised that most patients cannot wear retainers for the 2 to 3 years between phase 1 and phase 2.
I then discussed several areas and I would like to outline my points in this post and a further post next week. The first of these postings is concerned with dealing with uncertainty and denial of research evidence.
Dealing with uncertainty
In an earlier post I discussed the concept that research helps to reduce the uncertainty that is inherent in all clinical decisions. Paradoxically, this uncertainty is increased by people presenting clinical information based on low quality research and personal opinion.
When we consider reducing uncertainty on early class II treatment; we have evidence from several trials and a Cochrane systematic review. As a result, there is minimal uncertainty because this evidence suggests that routine early treatment does not provide any advantage over one course of treatment provided in adolescence in terms of; avoiding treatment, reducing complexity of Phase II treatment, the need for extractions and the final result of treatment. There is greater uncertainty about the effects on trauma and I will discuss this next week.
In spite of this evidence the subject is still felt to be controversial and I am not sure why. It appears that some clinicians simply do not accept the results of these studies and this brings me to the pyramid of denial.
The pyramid of denial
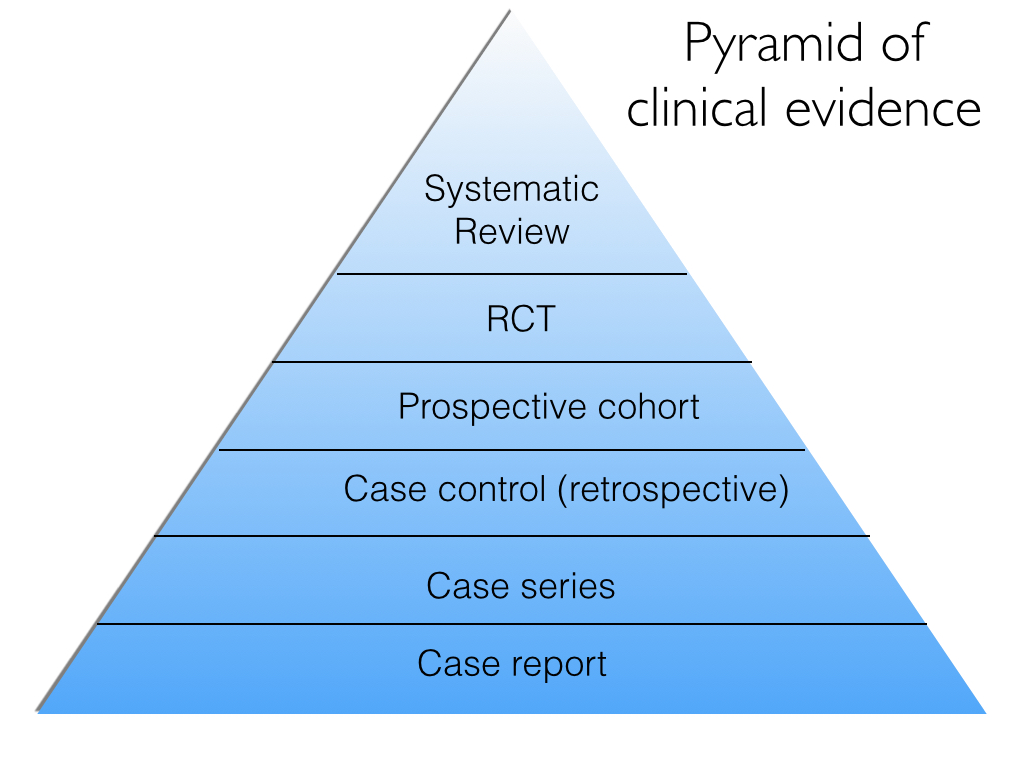
We are all familiar with the pyramid of strength of evidence that can help reduce uncertainty. For completeness I have inserted this in Figure 1.
Over the years I have debated the relative value of clinical trials and retrospective investigations. In these discussions several people have raised their concerns about the results and interpretation of randomised trials. I have decided to put these criticisms into a “pyramid of denial”. This is shown in Figure 2.
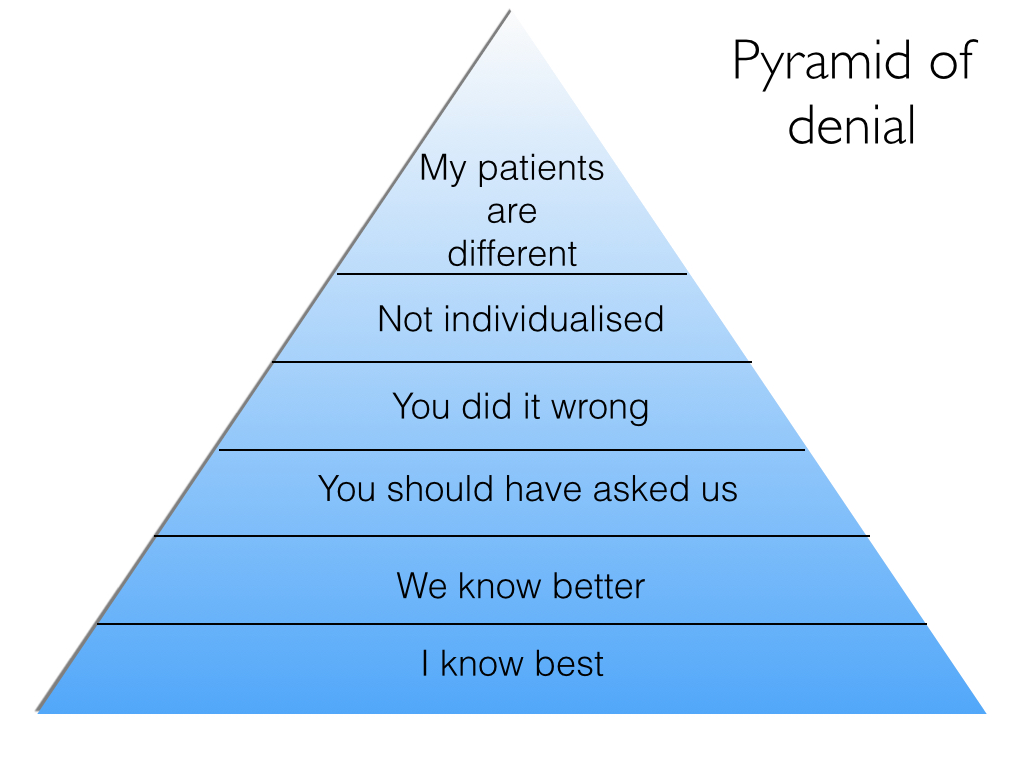
The base of the pyramid is anchored by the viewpoint that “we cannot believe the results of the studies because we know better”. This argument can be easily dismissed as it is the most basic level of denial and is based solely on personal opinion.
The next two layers are concerned with the opinion that the interventions were not applied appropriately, according to a person’s clinical experience. In other words they are suggesting that the clinicians who took part in the trial were not providing treatment “correctly”. This would mean that the clinicians were acting unethically. Again I find it difficult to accept this.
The next layer is that the treatments were not “ individualised”. This means that the investigators rigidly followed the study protocol and did not take the characteristics of the individual patients into account. This is rather unfair on the investigators. In any study the patient’s care should be a priority and while the investigators need to work to a protocol they also have to adapt their treatment in the best interests of the patient. If the interests of the patient are not considered the investigators are acting unethically. Furthermore, by providing care that is individualised the external validity of the trial is strengthened.
The final level of denial is that “my patients are different”. This means that their patients are so morphologically and genetically different from those in a trial that the results do not apply! There is really very little to say about this viewpoint except that it is very unlikely.
It is important that blog posts are relatively short and I will conclude this discussion next week in part two. “Early class II treatment: Part 2 evidence-based care and disappointment”.

Emeritus Professor of Orthodontics, University of Manchester, UK.
Hi Prof
I am currently an StR in Newcastle and myself and a colleague were fortunate enough to attend the AAO.
We were surprised by the approach adopted for early treatment and the lack of evidence to back it up.
The other point counterpoint lecture on prophylactic removal of 3rd molars (Given by residents) adopted a similar approach of we are aware of the evidence but we will do it our way anyway.
Thanks for the nice comments about our talk. I am very pleased with the feedback. I too am concerned at the problem of ignoring evidence, and I hope that I got my message over.
Dear Dr O’Brien,
I had the chance to listen to your presentation on the website link provided by the AAO. It is always interesting to read you; it was even more interesting to hear you! I agreed with you when you said something like: “I don’t understand why we are still talking about this…”. In fact, is there really a problem here? Treating early, waiting to treat in only one phase… Is there only one way to do things? The problem, with everything in life, is when it becomes a religion. You and Dr Sandler said it well: in the cases that were presented by Dr Dugoni and Dr Oh you would probably also have done a phase I treatment. The thing is, like my good friend Gerry Samson says: “There is not only one way to do things because, if it were the case, we would all be doing it!”. But I have a question regarding the RCT to be published by Dr Oh: on her table of results, they were showing that 38% of patient that had phase I treatment did not undergo phase II. The thing I missed is the reason for that. Was it because the clinicians saw no need to undergo phase II or is it because the parents saw no need to undergo phase II, as their chief complaint (teeth sticking out, bullying at school, etc…) were answered? How many of the 38% that did not do phase II, had it recommended by the clinician, meaning the parents refused treatment? Is this answered in their study? Thank you and please, keep up feeding this incredible blog! Entertaining and informative…
Thanks for the kind comment. I think that it is important to appreciate that the study presented by Dr Oh was not a RCT, it was developed from a selected sample of records from a retrospective study. It is also important to realise that this study has not been subject to peer review and published. As a result, I cannot really answer the question that you posed and it is a really good question.
Hello, Kevin.
This added Pyramid of Denial to your previous “uncertainty” post is thought provoking and appealing. My compliments on your point/counter presentation during the AAO, San Francisco. Due to standing room only status, I found myself sitting on the floor of the stadium waiting for the fire marshall to sweep me away. During your part of the presentation you mentioned more than once you were “saddened” by the debate of the Class 2 treatment timing topic. My impression was you felt it essentially a waste of time. However, you also underscored that complete informed consent is not possible without making parents (legal guardians) aware of evidence based agreements and disagreements. This was important, well stated and an essential reminder of our legal and ethical responsibilities. I continue to admire your hard work, always listen carefully, and have not found these efforts to waste my time.
Thanks Gerry, I will be dealing with consent in Part 2 of the post. Thanks for your support and publicising my blog
Dear Kevin is it possible to challenge the validity of the questions that You answer in your RCT without getting in the Pyramid of denial?
1 Is “Class 2” an homogeneous entity where we can always apply the same Strategy of Treatment and Criteria of Success ?
2 Do you think that the Inclusive Criteria of RCT for Class 2 reflect the “opinion” that Class 2 is an occlusal problem?
2 In a mixed dentition Class 2 where the diagnosis calls for extractions would you ever consider serial extractions or enucleations?
Could we consider this “early Treatment”?
I am always impatient to read your blog. Congratulations.
Renato
Hi Renato, yes it is possible to challenge the results of the trials without getting on the pyramid. this can be done by carefully looking at the science and applying tools, such as the Cochrane risk of bias tool. You have put forward some very good questions. I will try and answer them. I think that the best way to consider the definition of Class II is to define this as increased overjet. We did this in the Cochrane review. This is because there is a difference in the treatment of increased overrate and severe skeletal II discrepancy. It is also worth emphasising that a trial provides evidence of treatment on the average patient. As a result, if a patient is not considered to be an average patient, then the results of the studies are not relevant. However, it is important to identify the non average patients effectively and this clearly does not include all patients!
I have never done serial extraction in Class 2 cases and I am afraid that I cannot answer your third point.
I hope that these answers are OK?
Early treatment for class II and a lot of other diagnoses are some of the most prominent undead of orthodontic interventions. While they are mostly of poor performance, accompanied by high cost and long treatment duration, nonetheless many colleagues cannot withstand the temptation to treat early. As S. Jay Bowman joked in his special article (AJODO 1998;113:111-116): “(…McAndrew’s braces for baby teeth). Can in utero treatment be far off?… It is as if American children are suffering from SADS, systemic acrylic deficiency syndrome, given the popularity of housing large chunks of plastic in youngsters’ mouths.” Nothing to add to these words. Likewise bloodsucking vampires do not die unless a wooden pole is driven through their heart. In case of the vampires, it’s magic, in case of early treatment, it is the financial extra-profit which is the base for the uncredible longevity.
Despite I am a subscriber to 7 english-language orthodontic journals, some of them for as many as 25 years, I’m often amazed how concise and useful this blog is. In fact some good articles escaped my attention when first reading the journals and are nice re-discoveries after they were cited in the blog. Dealing with the most debated questions of clinical orthodontics, the best available evidence is summed up and presented. This is combined with a lot of pragmatism and clinical experience… simply great! I recommend this blog to my German colleagues and consider the last fifteen posts to be more useful than the last decade of the Journal of Orofacial Orthopedics/Fortschritte der Kieferorthopädie (official journal of the German Society of Orthodontics, but for some reason unread internationally). The blog is pragmatic and extremely useful for clinical work.
Thank you for your devotion to orthodontics and my compliments to Kevin O’Brien!
Thanks for your kind comments
I too was a big proponent of early treatment early in my career. When it worked it was nirvana but when it relapsed or had poor compliance it was hell and kept me up at night. No, it did not reduce the second phase significantly and I constantly heard “I have to have braces again” even though the parent & child were informed of two phases. Even my own daughter said those words. And the issue of wearing and keeping up with retainers between phases was a battle. I think some orthodontists made as much on replacing retainers as was the cost of the 1st phase.
Maybe in academia they have magical powers that the mere practitioner doesn’t possess but I doubt it.
Dear Dr. O’Brien
Kevin Boyd (Chicago pedodontist) here.
I just sent the following message (please see below) about your recent blog post to several orthodontist friends/colleagues and also to some ENT’s, paediatricians and pediatric sleep medicine physicians with whom I work very closely. I’d really like to talk with you sometime Dr. O’Brien about evidence from an ongoing trial we are producing at Lurie Children’s Hospital (Dept.Sleep Medicine) that shows compelling relationship between early/very early (some as young as 3 yrs old) non-retractive Tx (expansion and protraction) of class I,II and III pts. and mitigation of OSA symptoms.
I will be in the UK for a couple of days next month (30 June-3 July) per my anthropology research at U Penn and the London Natural History Museum and would really enjoy meeting with you if at all possible to discuss this aspect of indications for early intervention for class II malocclusion phenotypes.
Kind Regards
Kevin Boyd
message to colleagues:
Dear All- As evidence clearly shows that class II malocclusion and other malocclusion phenotypes are known to be associated with increased risk susceptibility to SDB/OSA, etc., I certainly hope at some point Kevin will address current evidences that clearly supports this. Perhaps he did so in an earlier blog post, but if not, maybe in part 2 Dr. O’Brien will also bring up the issues of airway health as being vital (literally) to the decision making process for when and how to treat, and also how to judge Tx success or failure.
Hi Kevin, thanks for the comments. I have never seen the results of any trial that addresses the issue of the airway and I cannot really comment on its importance. However, it is great to see that you are carrying out a trial into this, and I would really like to see the results. have you registered the protocol anywhere?
Dear Prof. O’Brien
Per your not having ‘never seen the results of any trial that addresses the issue of the airway’, please see the following:
1. “Sagittal airway dimensions following maxillary protraction: a pilot study”
Korkmaz Sayınsu, Fulya Isik and Tülin Arun
European Journal of Orthodontics 28 (2006) 184–189.
Conclusions
This study evaluated the effect of using maxillary disarticulation and protraction on the sagittal dimension of the naso- and oropharyngeal airways in 19 growing patients with a skeletal Class III relationship.
1. Point A moved anteriorly, the palatal plane showed a counter-clockwise rotation matching the clockwise rotation of the mandible as revealed by the decrease in SNB angle, and the vertical parameters showed a statistically significant increase.
2. The head was in a more extended position in relation to the cervical vertebrae. Nasopharyngeal airway measurements (PNS–ad1, PNS–ad2) showed a mean increase of 2.71 and 3.03 mm, respectively.
3. Maxillary disarticulation and protraction improved naso- but not oropharyngeal airways.
2. “Correlation between skeletal changes by maxillary protraction and upper airway dimensions”
Melsen, B.
Am J Orthod. 1975 Jul;68(1):42-54.
Conclusions
The nasopharyngeal airway dimensions can be improved in the short term with maxillary protraction in skeletal Class III children.
3.”Effects of maxillary protraction on craniofacial structures and upper-airway dimension.”
Hiyama S et al .
Angle Orthod. 2002 Feb;72(1):43-7.
Conclusions
These findings indicate that the superior upper-airway dimension can be altered during maxillary protraction
4. “Effects of Maxillary Protraction and Fixed Appliance Therapy on the Pharyngeal Airway”
Emine Kaygısız et al
Angle Orthodontist, Vol 79, No 4, 2009 p 660
Conclusions: In young individuals diagnosed with maxillary deficiency treated with reverse head- gear, the nasopharyngeal airway dimensions were improved after the treatment, and favorable effects of the treatment remained over the posttreatment period of 4 years.
5. “Obstructive sleep apnoea: a cephalometric study. Part I. Cervico-craniofacial skeletal morphology.”
Tangugsorn V1, Skatvedt O, Krogstad O, Lyberg T.
Eur J Orthod. 1995 Feb;17(1):45-56.
Abstract
A comprehensive cephalometric analysis of cervico-craniofacial skeletal morphology in 100 male patients with obstructive sleep apnoea (OSA) and 36 male controls was performed. The significant aberrations in the OSA group feature: (1) shorter dimension of cranial base with slight counter-clockwise rotation and depression of clivus; (2) shorter maxillary length with normal height; (3) maxillo-mandibular retrognathia related to nasion perpendicular plane (N perpendicular FH) despite normal angles of prognathism; (4) 47 per cent of the OSA group had mandibular retrognathia; (5) increased anterior lower facial height and mandibular plane angle; (6) reduced size of bony pharynx; (7) inferiorly positioned hyoid bone at C4-C6 level; (8) deviated head posture with larger cranio-cervical angle. Cephalometric analysis is highly recommended in OSA patients as one of the most important tools in diagnosis and treatment planning.
6. “Thin-plate spline analysis of treatment effects of rapid maxillary expansion and face mask therapy in early Class III malocclusions.”
Baccetti T1, Franchi L, McNamara JA Jr.
Eur J Orthod. 1999 Jun;21(3):275-81.
7. Changes of pharyngeal airway size and hyoid bone position following orthodontic treatment of Class I bimaxillary protrusion
Qingzhu Wanga; Peizeng Jiab; Nina K. Andersonc; Lin Wangd; Jiuxiang Line
Angle Orthod. 2012 Jan;82(1):115-21.
Conclusions: The pharyngeal airway size became narrower after the treatment. Extraction of four premolars with retraction of incisors did affect velopharyngeal, glossopharyngeal, hypopharyngeal, and hyoid position in bimaxillary protrusive adult patients.
Dr. O’Brien, while data from the aforementioned papers certainly do not come from what one might consider as ‘gold standard’ designed protocols (i.e., longitudinal prospective and blinded RCT’s), we nonetheless find the secular trends to be, as my former teacher ((g)Nathos 1995) and friend Gerry Samson says, ‘thought provoking and appealing’. And combined with what we are observing in our IRB approved clinical trial by having applied a scientifically validated dento-facial orthopedic Tx regimen (RME with/without mid-face protraction) in mitigating SDB/OSA symptoms in very young children with retrognathic maxillas and mandibles, it seems to us that the orthodontic profession is now perfectly positioned to improve the airway health of countless numbers of suffering children worldwide.
Thanks for the reply. I have had a look at these papers and none of them is a trial with clear findings. Can you let me know if your trial is registered and I can download the protocol?
Best wishes: Kevin
Thank you for another wonderful post. I too look forward to your comments regarding the orthodontist’s role in OSA to aid in drawing a line between reliable evidence and not so reliable evidence. I’m particularly interested in the link, if any, between OSA and four premolar extractions. Also, does maxillary expansion have an effect on OSA?
HI Joseph, Thanks for the comment and you raise a really good question. I’m not really aware of any trials that have been carried out in this important area. You have given me food for thought and I will do a posting on this at some point in the future.
Best wishes Kevin
Hi Kevin,
I am sorry I missed your presentation but I obviously agree with your suggestions.
I feel that it is disappointing to have to argue about the advantages of well-designed RCTs/SRs of RCTs over retrospective designs and part of the problem might be related to our curriculum.
Obviously, all types of studies have pros and cons but some have more pros than cons!
Bias is not something we can measure, however, proven methods that reduce bias, where possible, do exist and are often implemented in high quality RCTs. The key advantage of an RCT is the fact that it allows, when properly designed, to have a comparison between treatment groups which is fair. Therefore, if the only difference between treatment groups is the type of intervention then it is reasonable to assume that any differences between treatment groups is the result of the applied treatment.
We can infer generalizability by appropriate inclusion/exclusion criteria during the patient selection process. Again, as long as the treatment groups are different only in terms of the intervention [randomization applied] we have a fair comparison which will also produce findings applicable to other patients/settings.
I think what was happening at the exhibition halls was an indication of what may be driving our clinical decisions which brings us to your famous quote: “In the land of no evidence the salesman is king” or if I may add “in the land where we choose to ignore the evidence the salesman is king”
Perhaps, we need to examine the association between the size of the exhibition stand to the level of the evidence? I think one may find that this relationship to be inverse.
Your blog is a great contribution to the specialty.
Best wishes,
Nick
It all depends on what someone calls “early”. I see mention of treatment at 3 years, that really is early. However for some orthodontists early is anything before 28 permanent teeth have erupted (if there is room by then). Carrying out the main part of the growth guidance in the late mixed dentition has several advantages. The first is patient compliance and understanding. The second is that the arches are usually the correct shape at the end of that treatment, with sufficient room for all the teeth, making final torquing and leveling relatively quick and easy. Many of my patients were finishing their treatment just as their school friends were starting theirs. I am immune to the stability criticism because I, unlike most orthodontic practitioners, was able to monitor my patients for up to 25 years following the end of the active phase. I saw much more relapse, and more severe incidents, in extraction cases than maxillary development cases. One of the challenges in any debate on orthodontics is the lack of belief that most humans can be what we call Class I with the correct stimulus to growth. It is always possible to drag out cases of genuine micrognathia as in Pierre Robin, but the majority of patients are not so unfortunate.
There is the complication of unconscious bias that cannot be ignored. All of us, unless we have had specific training, will only see what we want to see. You only have to look at the carefully designed and seemingly honestly constructed studies purporting to support homeopathy to see this. A true doubly blinded study is impossible, so therefore all sorts of errors will creep in. I saw several references that practitioners “would have to be acting unethically” if they carried out certain treatments, and the idea that money might be a driver. These things might be true, but they also might be the sticks on the bonfire for those considered to be heretics.
Why don’t we accept that humans, like all mammals, should have their full genetic complement of teeth unless disease has intervened? In that case ALL orthodontics that does not result in 32 teeth in aesthetic and harmonious occlusion has to be considered a compromise. Severe lack of stability has to be admitted as a sign of failure in some way or other.
Dear Peter Crocker-I have followed your comments in recent months on Prof. O’Brien’s blog with heightened interest per our complementary interest regarding how the science of Anthropology can inform the science of Orthodontics. Your discussion from the April posting (Orthodontosis/Orthodontitis) mentioning how orthodontic Tx strategies should ‘mimic’ natural (pre-modern)processes (“As orthodontists we should attempt to mimic natural developmental processes. The maxilla is a membrane bone and requires stimulation to grow.”) was I think incredibly insightful in light of evidences from the Orthodontic and Anthropology peer-reviewed literature (references upon request). Over the past decade, and presently in my work as an anthropology student (back to school at 60 yrs. old!) and visiting scholar at the U Penn Museum of Archaeology and Anthropology(Philadelphia), I have been measuring what my dental anthropologist colleagues refer to as ‘pre-adult’ (i.e., no 3rd molars yet) crania from various parts of the globe over various eras in time (mostly pre-Industrial Revolution). The trend line is impressive Peter, that anatomically modern human (AMH) malocclusion is a relatively ‘recent’ phenomenon and it seems to have first appreciably entered the skeletal record around the time of the Industrial Revolution, and mostly near to your present dental office location. Our research group’s main question is centered around the observation that, after millennia of AMH’s/pre-AMH’s protection/freedom from skeletal malocclusion, it suddenly appears, first in central England, and mainly in nobility/gentry classes, but later within the Proletariat, and seems to coincide with changed infant/early childhood feeding practices as women began to enter as workers in the textile mills. Your point about ‘….we should attempt to mimic natural developmental processes’ is applicable here I think; specifically, in order for us to regain our genomic potential for erupted 32 teeth and associated healthy airway corridors, women do not need to go back to ancestral feeding and weaning practices, rather, the orthodontic profession needs to work collaboratively with other scientific disciplines (e.g., anthropologists, pediatric dentists and physicians, ENT’s Sleep Medicine docs et al) to find ways ‘to mimic natural developmental processes’ …..and that’s precisely why I am treating kids as young as 2.5 yrs old.
Hi Kevin.
Loved the pyramid of denial – brilliant!!
Dai
Good morning Kevin, I want to thank you for all you are doing for our profession. Your commitment to the literature / evidenced based dentistry is quite commendable and I thank you for your significant contribution(s) to our speciality.