What is the best treatment method for Anterior Crossbites: fixed or removable appliances?
A new trial of treatment methods for anterior crossbites
Every now and then someone publishes a paper that is directed at answering a common clinical question and they use simple straightforward trial methodology. Today in the EJO I came across this great simple study into the best method of correcting anterior cross bites. It was carried out in the University of Malmo, Sweden.
I am also pleased to see that the The EJO is rapidly improving as an orthodontic journal, as it is publishing more good quality clinical research and trials. However, the content is restricted behind a pay wall. I wonder if this could be changed and open access to the journal is provided? We’re looking at you European orthodontic Society!
Anna-Paulina Wiedel and Lars Bondemark
EJO 2015: 123-127. Doi:10.1093/ejo/cju005
What did they ask?
The introduction was very relevant and concise. They raised a very simple question which was
“Is it more effective to use a removable or a fixed orthodontic appliance to correct an anterior cross bite”.
What did they do?
They carried out a very simple randomised trial in which 64 patients were randomised to receive treatment either by a removable appliance or fixed appliance. Randomisation concealment and blinding were good. Two specialist orthodontists and a post-graduate student under supervision treated the patients.
The primary outcome measure was whether they corrected the cross bite. Secondary outcome measures were the treatment duration and dropout rate. They also collected outcomes on other dental measurements, but I am not going to go into these in this post. They collected data at the start and end of treatment and they analysed the data from all the patients regardless of the outcome.
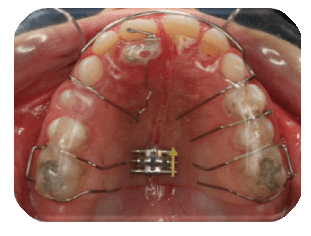
The removable appliance was a standard acrylic plate with a spring to procline the upper incisor. The fixed appliance was bonded to the anterior teeth and the primary molars or premolars, if they had erupted.
There was an adequate size calculation and the statistics were simple univariate tests. Although, if I was being very critical I would have liked to see a multivariate regression analysis. Nevertheless, they adopted simple outcome measures and the groups were matched at the start.
What did they find?
They randomised 62 patients into the two groups and all but one completed the trial. They found that all the cross bites in the fixed appliance group and all except one in the removable appliance group were corrected Therefore, in terms of the primary outcome measure there were no differences between the two treatments.
However they did find that the average duration of treatment was 1.4 months shorter with fixed appliance The average treatment time being 6.9 months for the removable appliance group and 5.5 months for the fixed appliance group.
The discussion was straightforward. It was clear that there were no differences between the two appliances. They also pointed out that the difference the length of treatment was not really clinically significant. I agree with them
What did I think?
I thought this was a really interesting and well carried out small study. It is also great example of how a common question can be answered with minimal resource and yet provide very useful clinical information.
If I am going to be critical(and I may being too critical?). One area that they did not evaluate was cost effectiveness, and I wonder if there was a difference in cost between the two treatment. I would also like to have seen some information on patients perceptions of the two appliances.
Will this change my practice?
Over the years I have used removable appliances to correct anterior cross bites and only occasionally used fixed appliances. I’m not really sure of the rationale behind my decision. Perhaps this was because I’ve always done it that way! I think from now on I will use more fixed appliances as it does seem more simple and straightforward in terms of treatment mechanics.
![]() Wiedel, A., & Bondemark, L. (2014). Fixed versus removable orthodontic appliances to correct anterior crossbite in the mixed dentition–a randomized controlled trial The European Journal of Orthodontics, 37 (2), 123-127 DOI: 10.1093/ejo/cju005
Wiedel, A., & Bondemark, L. (2014). Fixed versus removable orthodontic appliances to correct anterior crossbite in the mixed dentition–a randomized controlled trial The European Journal of Orthodontics, 37 (2), 123-127 DOI: 10.1093/ejo/cju005

Emeritus Professor of Orthodontics, University of Manchester, UK.
http://www.angle.org/doi/pdf/10.2319/041114-266.1
Stability of anterior crossbite correction: A randomized controlled trial with a 2-year follow-up
Anna-Paulina Wiedel, Lars Bondemark
This is very useful information, thank you and I certainly applaud and underscore your request to have the EJO in open access format.
Hi Gerry, thanks, I would really like to see all orthodontic journals in open access format.
I love your Blog! I really enjoy reading each topic!
Evidently Swedish children are more compliant with removable appliances than American children! After many compliance issues I only used fixed appliances. Either a fixed 2X4 or 2 X 2 appliance with a continuous archwire with offsets distal to the laterals to jump the crossbite or if the x-bite was too deep for brackets or parents didn’t want occlusal build ups to open bite, I would use a quad-helix with lingual sweep arms to the tooth in crossbite and bonded a lingual ledge of composite material to prevent the arms going above the incised edge. Most crossbites were corrected in less than 5 per 6 months as in article.
I learned these techniques from my good friend Gerry Samson, Marietta, GA, USA.
Does anyone here have experience with a fixed mandibular inclined bite plane? I have read that it fixes crossbites the most efficiently but do not have any personal experience using them. Compliance is not a factor because the biteplane is bonded in to the lower molars.
regarding fixed mandibular bite planes I have used a small composite addition placed to the upper incisor which are in cross bite, the composite is shaped to make it wedge shaped. The cases I have done it on have worked very well, I used them in the very early mixed dentition when the upper centrals had just erruted in cross bite when the overbite is not fully established and the cross bite was causing a forward dispalcmenet. Only done it around 4-5 cases when I think it would work and in all cases worked in a few weeks. takes 2 mins clinical time and patients tolerated it well.
I have used the technique of bonding the incline to the maxillary incisor dozens of times and been very pleased with the results. The advantage is not only cost and time, but you also get movement of both the upper and lower incisor. It can also be used on cuspids and tipped bicuspids
i think that the effect of Fixed or Removable Appliance is differ acording to:- the nature of the anterior crossbite ( Skeletal or dentoalveolar), – the etiology ( environmenal, functional or Genetic factors) – and the Age of patient
This a very interesting results but I think that the treatment outcome depends on the patient cooperation
Hi Kevin,
On your blog you wrote: “One area that they did not evaluate was cost effectiveness, and I wonder if there was a difference in cost between the two treatment.”
And then, one week later, on May 4th, 2015, this comes out in Eur J Orthod:
A cost minimization analysis of early correction of anterior crossbite—a randomized controlled trial.
Anna-Paulina Wiedel , Anders Norlund , Sofia Petrén , Lars Bondemark Eur J Orthod (2015) DOI: http://dx.doi.org/10.1093/ejo/cjv026 First published online: 4 May 2015 (6 pages)
Seems you are in direct spiritual connection with the authors! 🙂
Best, Spyros
Yes, it was nice to see this. I will post about this in a couple of weeks, when I get back from the AAO congress
i really don’t find any research who used fixed appliance without bite plane for correction of anterior dental cross bite.
I was interested in your comment about EJO content being behind a paywall – but isn’t that true of many journals? I appreciate some have free access, but what model would be better to cover their costs of running the journal, even if there was never a paper copy? You have some form in the area I presume because you ran BJO – do these things cost much to make? Do advertisers do well out of a digital copy?