Align Technology responds to my post about Invisalign Mandibular Advancement
Last week I posted about Invisalign Mandibular Advancement. Invisalign felt that some of my statements were not correct. As a result, I offered them a post to address their concerns.
This has been written by Dr Beena Harkison, she graduated in Dentistry from the University of Witwatersrand. She has a post-graduate qualification in implantology. She joined Align Technology in 2007 and is now Director of Clinical and Professional Education for Europe, Middle East and Africa (EMEA).
I would like to take the opportunity to comment on your recent blog post about one of our recent innovations, Invisalign Treatment with Mandibular Advancement. We realise that you and your readers have some questions regarding the aligner feature which I will address and I’d also like to clear up a few misconceptions that we saw in your blog post.
Introduction to Invisalign Mandibular Advancement:
Invisalign Treatment with Mandibular Advancement is a clear aligner solution for Class II correction in growing teenage patients. It is aimed at patients between 11-16 years old in the growth spurt that present with retrognathic Class II malocclusions in a permanent dentition or in a stable late mixed dentition (stable E’s are necessary during the mandibular advancement [MA] phase), as per the descriptions below:
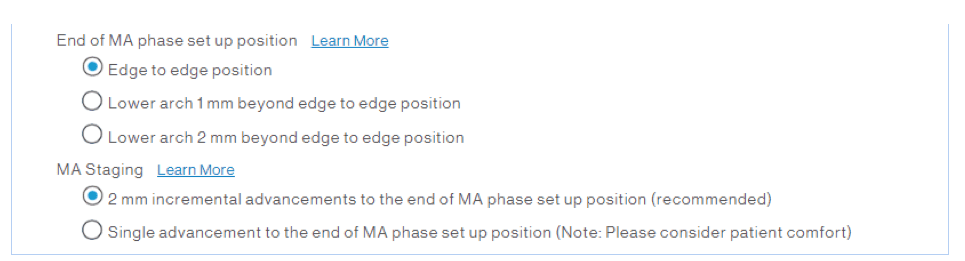
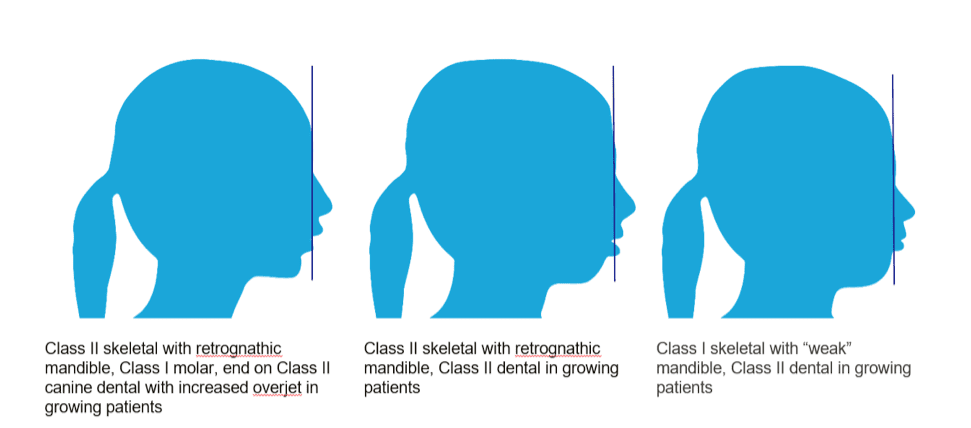 This new offering combines the benefits of advancing the lower jaw forward while simultaneously aligning the teeth. The Class II correction can be achieved in single or multiple jumps as indicated in the prescription form (or through the ClinCheck plan modifications) by the treating doctor. Doctors can select to either stage the MA with 2mm incremental advancements (every 8 stages/aligners) to the end of the MA phase or may choose a single advancement to the end of MA set-up position. For increased flexibility, doctors can also select their end of MA position as edge-to-edge or the lower arch to be 1 mm or 2mm beyond the edge to edge position.
This new offering combines the benefits of advancing the lower jaw forward while simultaneously aligning the teeth. The Class II correction can be achieved in single or multiple jumps as indicated in the prescription form (or through the ClinCheck plan modifications) by the treating doctor. Doctors can select to either stage the MA with 2mm incremental advancements (every 8 stages/aligners) to the end of the MA phase or may choose a single advancement to the end of MA set-up position. For increased flexibility, doctors can also select their end of MA position as edge-to-edge or the lower arch to be 1 mm or 2mm beyond the edge to edge position.
A screenshot of the prescription form for MA is below:
Additionally, doctors can prescribe additional techniques and mechanics to support a full CII correction in the following scenarios:
- Severe, full cusp Class II malocclusion > 6mm may require Class II elastics.
- Dolicho-facial/vertical growth patients, open mouth breathers may require vertical elastics.
- Grinders may require vertical elastics and extra vigilance on wing engagement.
Current data:
Invisalign Treatment with MA was clinically evaluated in a multicentre prospective IDE Clinical Study in North America. 10 clinical sites were involved in the study, and 40 patients were analysed. The average patient age was 13.2 (±2.1). 53% of the patients were male, 47% female. The study methodology included before and after records (photos, study models and radiographs), a pre- and post-treatment Quality of Life Survey and cephalometric analysis (completed by a third party; University Faculty). The average number of MA aligners/arch = 36.3 (±17.3) and the average MA phase was 13.4 months (±5 months). Cephalometric analyses were also completed for the 40 patients (outlined in the table below):
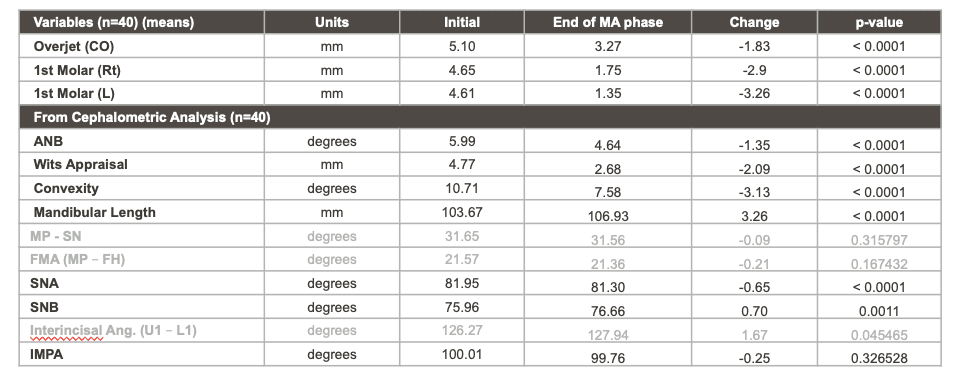
The table above demonstrates the dental changes (1stMolar Rt, 1stMolar L and overjet) and skeletal changes (SNB, ANB, Wits Appraisal, Convexity) that were seen, all of the values with p-value < 0.0001. Additionally, IMPA showed limited lower proclination. Thus, demonstrating that Invisalign clear aligners with MA can effectively treat CII malocclusions in growing patients. To date, over 17,000 teenagers have used Invisalign with the mandibular advancement feature. As we continue to add more data to this IDE study (and from the 17,000 treatments in progress), we hope that we will be able to present this to you in a future blog.
For those that are interested in learning more about Invisalign Treatment with Mandibular Advancement, the link below will re-direct you to a webinar hosted by one of the principal investigators of the IDE study, Dr Barry Glaser, accompanied by Dr Milos Lekic.

Emeritus Professor of Orthodontics, University of Manchester, UK.
Where is this multicentre study published? I miss the citation.
Please provide some characteristics of the control group. How was the matching done? How did you account for the effect of growth on the ANB, and the effect of E-space in molar correction? How was the quality of the result evaluated? Was the ABO-OGS criteria used?
Am i missing something?
An initial mean overjet of 5.10mm and a mean 1.83mm reduction? Also, as all K-O’B-B readers know, just because it is statically significant does not mean it is clinically significant.
We await the published RCT…
The mean initial OJ of 5.1 is rather low and essentially normal. If this is the mean then presumably half the cases have OJs below this.
All the evidence supports the current opinion that we cannot grow jaws so can we please stop claiming that we can. If you must use a functional then I would imagine that the invisalign one will work as well or as badly as any other, provided it doesn’t break. But maybe there’s a better way to treat patients than the functional appliance.
good point
-1.83mm of overjet reduction and -1.35 of ANB reduction are really poor results for a CLII treatment approach as compared to the many data appeared in the literature. Even without control group the attentive reader may induce that this MA feature appears to be an at least doubtful CLII corrector. I guess that clinical research performed and presented by the Aligntech company should be revised by some academics before to present as supportive of their system. Indeed this research claims that the MA is a scanty CLII corrector…
Normal growth changes were not accounted for. This seems to be a series of cases report. Is the data of all cases started?
These appear to be normally growing individuals (see MP) so that should also be considered as results do not have full external validity.
It is interesting that mandibular incisor inclination was not only maintained but improved.
As mentioned before initial OJ is not representative from a significant Class II.
SD data would also be useful to calculate CI values.
17,000 patients…that should be interesting to see the details of the data…if they ever come out.
Recognizing that Dr. O’Brien is by no means a raving fan of cephalometric data still, this report is suspicious. The cephalometric table shows mandibular length increase (improvement) of 3+mm, convexity reduction (improvement) of -3mm and positive Wits change of -2.09mm. All of this within a treatment time of 13.4 months (±5 months) – a remarkable improvement. However, these data are not in agreement with the lack of SNB improvement of +.70 degrees which is not significant and within measurement error. On this side, I am curious as to how Dr. Harkison can resolve this apparent contradiction.
There is no reason to wait for RCT. I can tell you that it will easily stand in any RCT study. (Disclosure: I use Invisalign to cases where I understand it will work – some tipping and no whatsoever torque). Now imagine that you apply by whatever you want, a palatal force on the upper jaw will it be by 2 bite plates or aligners, by positioning the mandible forwards. This by itself develop both backward force on the upper teeth and forward force on the lower teeth. If this last, 13.4 month, it will be amazing not to get the results they show, especially if during this time they resolve some lower incisors crowding. Wouldn’t you expect the lower incisors to dump forward and the upper a bit backwards, will not this affect the ANB and the WITS. The major effect of the Clark appliance is more than we see here. It controls and changes the occlusal plane and this cannot be achieved with the aligners. Ceph numbers’ changes can be very convincing however if you understand what is behind the numbersyou find it meaningless.
One point that this appliance taught me about the system: No movement with the aligneres is safe. Lately I heard a lecture from an aligner’s heavy duty user that tried to convince the audience telling that there is no loss of anchorage using aligners. Well, there is no action without reaction and no force without loss of anchorage. Therefore we are still far from understanding those appliances, and as we are in the 6th generation now, I believe that the 7th and further generations are on their way.
I fully agree that more/better studies are needed. However in orthodontics this is very difficult. In Germany the state questions the advantages and effectiveness of orthodontics altogether and has commissioned a study released in November – outcome: we need far more good studies (RCT) and more guidelines. This may be intended to remove orthodontics from the social insurance system. The trend is now: no RCT’s (including untreated controls!) means all you do is useless….no matter how many cases we show of patients who in our opinion benefited enormously from our treatment
It would not be the first government to be selective and massage ~ adept with data to produce evidence for reducing expenditure .!!
I ,regretfully,believe that one is able to design studies to show the very outcome you desire ,in many cases.
You may want to look at the British NHS which has a “severity “index to determine what complexity level of cases they wish to financially “cover “.
I have experience of ortho in Canada ,UK,Austria and Germany.
The German government may be doing you ,as a clinician ,a huge favour in “delisting “such services.Probably you will see less pts ,have less stress and increase your income !Just a thought.
Like many socialist leaning governments ,German government may be running out of other people’s money LOL.
This reply brings up more questions regarding the “evidence” than it answers. Can we please see the published study instead of seeing a very simplified reply that basically says, “use it because our paid and perhaps biased KOLs with books to sell and lectures to present say it works”?
I cannot help but question the entire study when the sample of 40 teeanage patients chosen (from the stated 17,000 patients treated with this MA device) are of an average age of 13.2 years old (+/- 2.1 years). Is this the age at the start, middle or end of treatment?
If it is the age at the start of treatment (as seems to be implied) why would you pick your sample for a functional appliance growth study to include patients that are already an average of 13.2 years of age (and apparently as much as 15.3 years of age)? It’s a lot to ask a 15 year old female mandible to grow more quickly than normal with little or no growth remaining at all. Why not pick a sample that includes patients that are at a more commonly perceived age in which there is likely on-going growth?
Publish please!
We all know its possible to move teeth with aligners in teenagers, but why would anyone want to ? 36 aligner stages delivered over the many months of care is an extraordinary number of aligners and creates significant complexity in the clinical setting for the patient doctor and staff. As a profession, I hope we continue to question the practicality of using an aligner system, any aligner system, that offers a cookie cutter mentality to treatment. Being able to customize care to our patients with the myriad of tools we have available seems more practical and efficient for all involved. And limitations of plastic moving teeth in specific biomechanical situations (axial inclination, bodily movement, extrusion, etc) are well documented. Clinicians need to choose the right tool for the job at hand. Golfers get to choose from 14 clubs in their bag. No one would ever consider playing with only one, at least not if they were hoping to achieve a quality result.
I too would love to see the citation of where this information was published, but as several comments have noted, the A-P correction is not spectacular nor insightful. Elastics move teeth a certain way. Orthodontists know this and have known this for decades. Lets see this for what it is: an interesting clinical trial demystifying elastic wear with aligners so non-specialty trained doctors or do it yourselfers can fix overjets.
This aligner company is using big data (mining the clinical data that orthodontists have been sending for 2 decades now) to build the case for using aligners for every clinical situation and eventually removing the doctor from the picture entirely. Their business model is clear. The “no doctor aligner stores” are opening all over the country and our legal system has not been able to stop them.
Could not agree more!
I am very interested in seeing CBCT images of lower incisors in the bone trough in facial to lingual reconstruction. Remember the patient has either a thin or a thick biotype. For long term periodontal health the incisors need to be in best bone possible. Let’s see the reconstruction!!!
Agreed!
In early mixed dentition the maxilla grows forward by 1.1 mm/year and the mandible by 2.6 mm/year : the difference is 1.5 mm.
During growth spurt the maxilla grows forward by 1.4 mm/year and the mandible by 2.8 mm: the difference is 1.4 mm
Conclusion : during adolescence, waiting about 2 years and just dong nothing, we can normally observe the same changes as in the Invisalign data above. These are basic data from many growth studies by Franchi, Baccetti, Mc Namara, O Brien etc. Oh please , researches, don’t loose your time and our public money with other studies of the magic effects of this plastic marketing. There is nothing new under the sun about functional appliances. and I used most of them. Supplementary growth of the mandible varied widely among studies, but it exceeded never more than 3 mm , and only mentioned in 30% of all studies. Please let us be honest and brave , as was Cicero 2000 years ago against his offender Cataline :
Quosque tandem abutere, Catalina, patientia nostra ? How long are you going to try our patience Invisalign ?
Yet another poorly reported data set from a company wanting to sell a product.
Do they really think a start overjet of just over 5mm is “severe”.
All this data show is that during the period of appliance use the children grew. I think if they also measured the patients height and voice characteristics they could also prove that Invisalign mandibular advancement will make you taller and deepen your voice.
A few thousand dollars and a significant amount of patient/parent investment for ? nothing other than company profit. Is this what orthodontics is becoming.
could not agree more , great comment…
” 10 clinical sites were involved in the study, and 40 patients were analysed”
I can’t find any study registered on “clinicaltrials.gov”. Seems to me it should be.
Also, is is 4 patients per 10 clinical sites for a total of 40? Is a “clinical site” the office of a KOL? Just curious
would Invisalign like to present the data from their pre-launch trial (which I presume was outside the USA)?
How many cases were treated with this before they went to market with it?
How much has that appliance changed since then, or are the 17000 treated since (that’s only over a few years, which is impressive) using essentially the same appliance?
Stephen Murray
swordsortho.com
I noticed in this discussion thread a theme of skepticism regarding how research can inform practice. It is an old saw that NED does not equal END (no evidence of disease is not the same as evidence of no disease). Those who would not use aligners for mandibular advancement mistakenly justify their personal practice policies by noting (correctly) that good multiple publications are years away. An open mind might be a better posture.
Invisalign has done what is expected in the professional community by gaining approval from the U. S. Food and Drug Administration for a substantial equivalent dental device in advance of marketing their MA system. The requirements for 510K approval are in many ways more rigid than those applied to papers published in the literature. The testing standards are posted on the FDA website. The approval document can be seen by searching “FDA K181739.” The federal approval states: “Clinical Testing. Align conducted an FDA-approved, endpoint driven clinical study for the Proposed Device at multiple sites to demonstrate clinical safety and effectiveness, and to gather data for marketing claims. The results of the study confirm the Proposed Device is a safe and effective means of correcting skeletal and dental class 2 malocclusions. No adverse events occurred in this study.”
There should be no confusion between claiming that a device (intervention) is safe and effective and that it is the best one for a given orthodontist to use. Research might warn against using some approaches, but even systematic reviews and meta-analyses will likely always be chasing practitioners’ professional judgment. A useful reference in this regard is Lee, R., MacFarlane, T., and O’Brien K. Consistency of orthodontic treatment planning decisions. Orthodontics & Craniofacial Research, 1999, 2 (2), 79-84. The lesson in that article is that orthodontists will pursue widely diverse personal practice preferences in the face of research evidence.
I have no affiliation with Align Technologies.
Well said
I would like to thank the readers for their questions and comments. I am more than happy to address these offline and can be reached on [email protected].
A -1.35 of ANB reduction, can be from growth, or tracing bias, or both. Not a great study.