Dentistry and Covid-19 Antibody Testing
I have previously posted information on dentistry in the post-COVID situation that the excellent Dental Elf site has published. Mark Howe wrote this latest post on antibody testing. It is very current as the UK government has just approved an antibody test. I thought that his post was very clear and sensible. I have adapted it for my blog.
Introduction
As we are acutely aware, the whole country has been locked down in an attempt to reduce the spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2 (Covid-19)). At the same time, we restructure the healthcare systems and direct research funding into treatment and/or a vaccine.
The next stage is to rapidly scale up diagnostic testing. We need to collect robust base-rate data at both an individual and population-level for future high-quality decision-making (Ioannidis, 2020). Importantly, we need to know who has been infected. This information is particularly important for dental care professionals because of the potential risk of Covid-19 spread via aerosol-generating procedures (Coulthard, 2020). So what is the current state of affairs regarding quick point-of-care antibody testing? How good is it, how good should it be, and why is this important?
Firstly, I am going to use a recently published paper that evaluated 10 antibody tests for SARS-CoV-2 using Enzyme-Linked Immunosorbent Assay (ELISA), and Lateral Flow Immune Assay (LFIA), lateral flow assay. These utilise the same technology commonly used for pregnancy tests (Crook, 2020). This particular paper has sparked a considerable controversy which I will go into later. If you need more detail on how these tests work and their advantages/disadvantages, then please take a look at the Oxford COVID-19 Evidence Service (Green et al., 2020). When looking at diagnostic accuracy testing the two main concepts to understand are:
Sensitivity – The ability of a diagnostic test to give a positive result when it is supposed to be positive.
Specificity – The ability of a diagnostic test to indicate a negative result when it is supposed to be negative.
Results
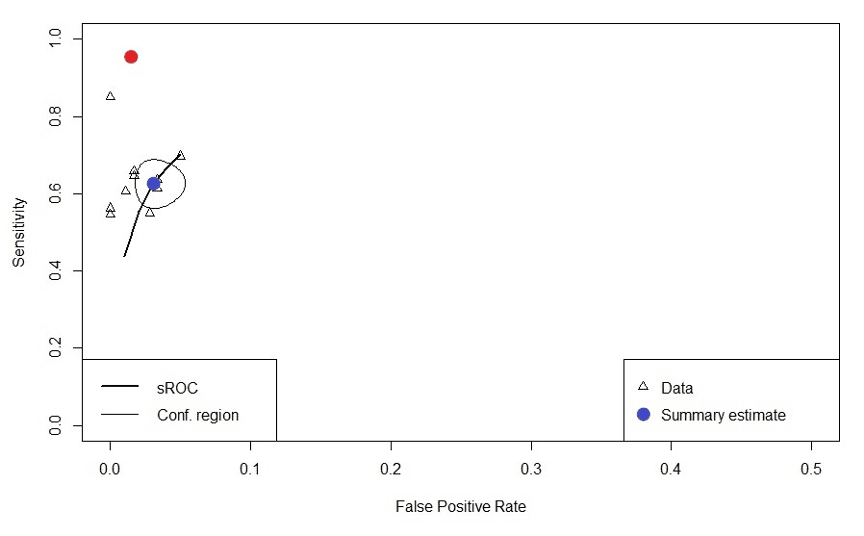
After I extracted the primary data from the individual tests, I did a meta-analysis using the ‘Mada’ package in R. I found that the summary estimate for sensitivity was 62.7% (95%CI: 57.5 to 67.7) and specificity 96.9% (95%CI: 95.2 to 98.0). I then plotted the results for the ELISA test and the 9 LFIA tests on to a Summary Receiver Operating Characteristic (sROC) curve ( See Figure 1). The y-axis is the sensitivity (1.0 =100%), and the x-axis is 1- specificity (0.10 = 10%).
For a test to be perfect, the summary estimate point should be in the top left corner representing 100% true-positives and 0% false-positives. The blue dot represents the summary estimate for the tests surrounded by a 95% confidence area, the red dot represents the specification target of >98% (95%CI: 96 to 100%) for sensitivity, and >98% (95%CI: 96 to 100%) for specificity, set by the Medicines & Healthcare Products Regulatory Agency (MHRA., 2020).
Figure 1. sROC curve – Antibody tests
Discussion
So why is so important to set the levels of sensitivity and specificity so high for antibody testing? Imagine we have a small city with a population of 100,000. The prevalence of people who have had the virus and recovered is 6%. If you are using an LFIA test with a sensitivity of 63% and a specificity of 97%. Out of 6600 people who test positive for virus antibody, only 3780 are true positives which correspond to 57% having a correct positive diagnosis (See Figure 2.). Furthermore, another important consideration is that 3% of the population who do not have antibodies test positive (n= 2820) and could lead them to believe they are immune.
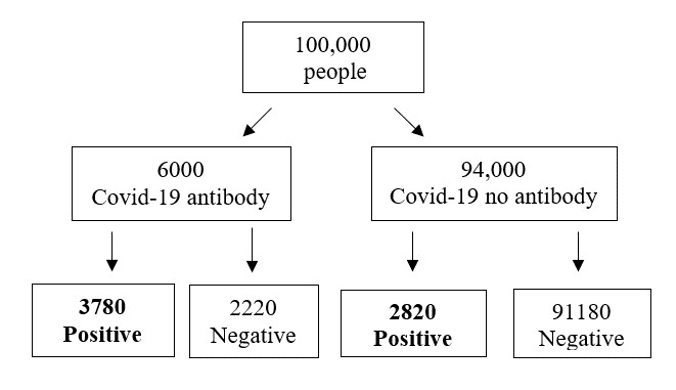
Figure 2.Frequency tree of Covid-19 antibody screening
The second point about this paper is that in its present format, it cannot be used in any future analysis. This is because the companies that supplied the tests required a commercial confidentiality agreement to be signed with the UK Department of Healt. This made it impossible to discriminate between tests.
Unfortunately, the current set of results show poor performance. As a result, the MHRA has set its targets high. This is because of the risks that results could pose if they were used to ease a lockdown, or they become part of an immunity passport system (Mahase., 2020; WHO, 2020).
Finally, whenever we have to deal with diagnostic tests or screening devices in our professional or private lives we need to be able to identify the products, their comparators and their accuracy before making a decision to use or purchase the product. Importantly, false-positive and false-negative results can pose significant harms to both ourselves and the population.
References
COULTHARD, P. 2020. Dentistry and coronavirus (COVID-19) – moral decision-making. Br Dent J, 228, 503-505.
CROOK, D. W. 2020. Evaluation of antibody testing for SARS-CoV-2 using ELISA and lateral flow immunoassays [Online]. Department of Microbiology, John Radcliffe Hospital, Oxford, OX3 9DU, United Kingdom. [Accessed].
GREEN, K., , A. W., DICKINSON, R., GRAZIADIO, S., ROBERT WOLFF, MALLETT, S. & ALLEN, A. J. 2020. What tests could potentially be used for the screening, diagnosis and monitoring of COVID-19 and what are their advantages and disadvantages? [Online]. Available: https://www.cebm.net/covid-19/what-tests-could-potentially-be-used-for-the-screening-diagnosis-and-monitoring-of-covid-19-and-what-are-their-advantages-and-disadvantages/ [Accessed].
IOANNIDIS, J. P. 2020. A fiasco in the making? As the coronavirus pandemic takes hold, we are making decisions without reliable data [Online]. STAT. Available: https://www.statnews.com/2020/03/17/a-fiasco-in-the-making-as-the-coronavirus-pandemic-takes-hold-we-are-making-decisions-without-reliable-data/ [Accessed].
MAHASE., E. 2020. Covid-19: Confidentiality agreements allow antibody test manufacturers to withhold evaluation results.
MHRA.2020.Target_Product_Profile_antibody_tests_to_help_determine_if_people_have_immunity_to_SARS-CoV-2_ [Online]. Available: https://www.gov.uk/guidance/guidance-on-coronavirus-covid-19-tests-and-testing-kits [Accessed].
WHO.2020. “Immunity passports” in the context of COVID-19 [Online]. Available: https://www.who.int/news-room/commentaries/detail/immunity-passports-in-the-context-of-covid-19 [Accessed].

Emeritus Professor of Orthodontics, University of Manchester, UK.
Thank you Kevin,
How are the results changed if repeated tests are used? I.e. the chances of being falsely positive or falsely negative in repeated tests.
Would this improve or confuse the situation?!
Best wishes
Adrian