Let’s talk about myofunctional orthodontics…..
Let’s talk about myofunctional orthodontics….
In this post, I would like to provide my academic opinion on the interesting, yet controversial, area of myofunctional orthodontics. I have been prompted to do this following feedback on previous blog postings from those who have developed and promoted the concepts of orthotropics and myofunctional orthodontics. I have also spent some time researching the background of this subject and I would like to discuss these, interesting, related concepts together in one post.
Where do we start?
A good place to start is to consider that if malocclusion is a disease (and I am not even sure if this is correct) then orthodontic treatment should be directed to correct its aetiology. But as we all know, the aetiology of malocclusion is not clear and the most widely accepted theory is that malocclusion has a genetic and environmental aetiology. For example, if we consider a person with a skeletal II malocclusion, we suggest that the skeletal component is genetically determined and the position of the teeth is modified by the environment of the soft tissues. This whole concept is covered in standard sources and particularly well by Bill Proffit in his classic paper “Equilibrium theory revisited”. I have discussed this in this post.
While this may be accepted knowledge and appears to be logical; the strength of evidence underpinning this concept is not high and is mostly supported by personal opinion and theory. I still remember the many hours I spent trying to understand Moss’s functional matrix and Bjork’s papers on facial growth! As a result, other theories exist. One of these is that the influence of the environment is the major (or only) aetiological factor. In effect, the environment has influenced the position of both the skeletal bases and the teeth. This leads to the hypothesis that it is possible to “cure” malocclusion by correcting the environment. This may be achieved by providing treatment when patients are young with the aim of changing the soft tissues and the airway. Furthermore, because the cause of the malocclusion has been removed the treatment will be stable. Proponents of this philosophy suggest that this is different from treatment with fixed and functional appliance therapy, which merely masks the malocclusion by moving teeth and the actual cause of the malocclusion is not addressed. In many ways, this concept has a degree of logic But before you start thinking that “he has lost the plot” then read on…….
Is this a new concept?
It is important to remember that little in orthodontics is new, and many ideas and concepts are simply recycled from time to time. It is certainly established practice in some countries to provide orthodontic treatment with muscle exercises. Indeed, the whole concept of Frankel’s treatment was based around altering the muscle balance around the teeth. But let’s look at these treatments in more detail. I am going to discuss orthotropic and myofunctional braces together because I feel that the concepts are related, nevertheless the appliances are different.
Orthotropics
This form of treatment was developed by John Mew in London, South of England. Over the last 15 years I have had many discussions with John about his ideas and treatment, and he has given a seminar to the specialty trainees at Manchester. There is no doubt that his ideas have not been accepted by UK orthodontics and there may be many reasons for this and I do not want to go into them now. He has recently been joined by his son, Mike, who is a specialty trained orthodontist and these ideas are being put forward in a concise way. Details of this treatment are on their website.
In brief, orthotropics is based around the theory that different forms of removable appliances, along with relevant muscle training, correct the soft tissue behaviour and oral environment. This then results in the development of the skeletal bases and change in the position of the teeth. I have looked at the evidence that has been published and unfortunately I could not find any sufficiently powered prospective studies. He illustrates successfully treated cases in papers, a recently published book and on the website. But some of these look a little dated. This is perfectly reasonable because John has been working as a single handed practitioner for many years with limited resource. Nevertheless, there is not doubt that some of the results are impressive.
Myofunctional orthodontics
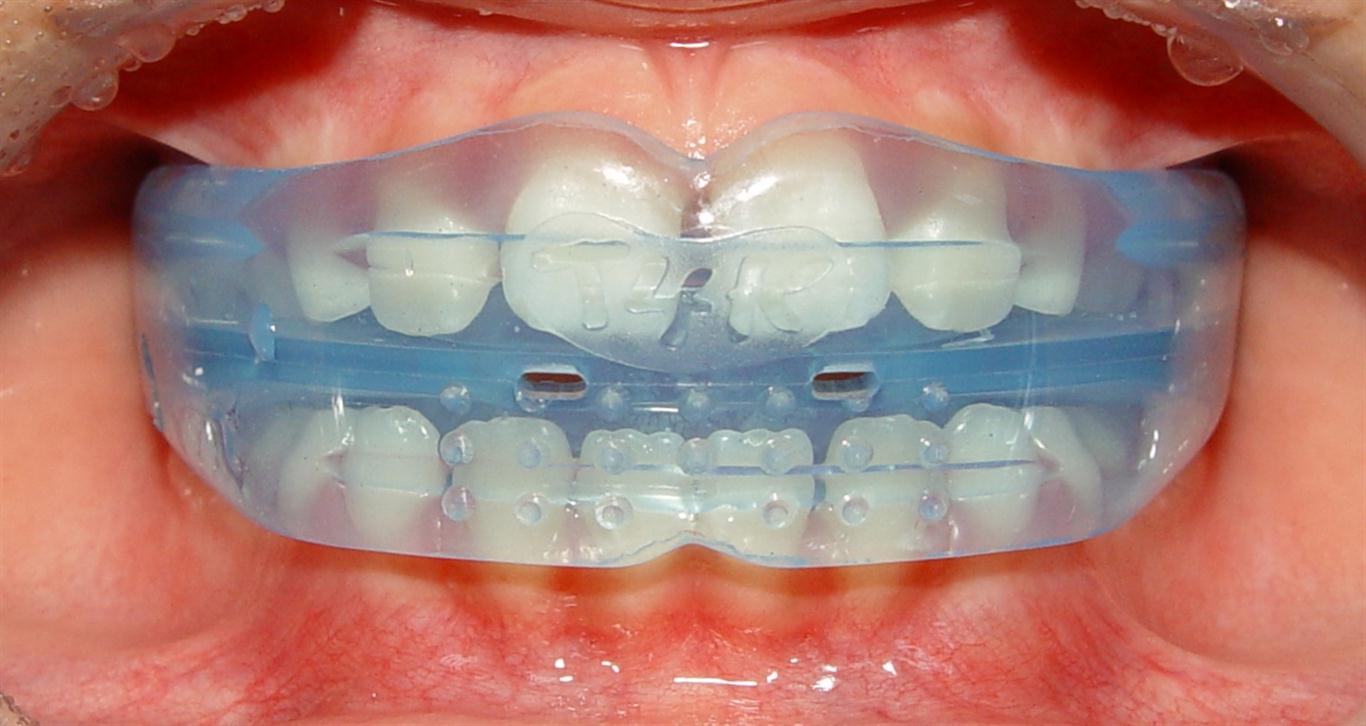 This is a relatively new treatment, that has been influenced by the thinking of John Mew, and again this is based on correcting the soft tissue pattern early. One of the largest providers of this treatment are Myofunctional Research Co. The really interesting aspect of this treatment is that different appliances are used for different malocclusions and ages of patients and the appliances are not custom made. They are “taken off the shelf”. I think that this is a really interesting concept. Their website is very well presented and professionally built, and can be found here. They show many treated cases and highlight several publications that support their treatment concept and philosophy.
This is a relatively new treatment, that has been influenced by the thinking of John Mew, and again this is based on correcting the soft tissue pattern early. One of the largest providers of this treatment are Myofunctional Research Co. The really interesting aspect of this treatment is that different appliances are used for different malocclusions and ages of patients and the appliances are not custom made. They are “taken off the shelf”. I think that this is a really interesting concept. Their website is very well presented and professionally built, and can be found here. They show many treated cases and highlight several publications that support their treatment concept and philosophy.
When I reviewed the cases, I thought that they were interesting, but most of the photographs were confined to anterior and occlusal views, there were only a few with buccal shots illustrating the posterior occlusion. The papers that they included were, in my academic opinion, mostly low scientific quality retrospective studies that measured muscle force or cephalometrics. They were chararactised by lack of power calculations, inappropriate statistics, multiple comparisons and discussions about small effect sizes. Nevertheless, these were published in refereed journals such as the Angle Orthodontist and the European Journal of Orthodontics. While I may be critical of the methodology etc, there is no doubt that the quality of these studies are at the same low level as some published research into more conventional orthodontic treatment. However, one paper could be important and this was the study by Keski-Nusala et al. in which they used an eruption guidance appliance. I have previously reviewed this paper and found it very interesting and relevant.
Finally, when we consider that the appliances can be fitted without impressions, this makes them readily accessible to the general practitioner.
So what do I think?
This is difficult, mostly because of the “white noise” and confusion surrounding these therapies. If I could treat my patients with removable appliances and achieve results that were more stable with a lower failure rate than fixed appliances I would embrace this concept completely. If the treatment could be provided by general practitioners this would be even better, as it would increase access to orthodontic care. But I will not be convinced that this is an effective treatment until I have seen studies that report a higher level of evidence. I am also more interested in studies that provide information on the alignment of the teeth, the burden of care, co-operation rates and the final results of treatment, as opposed to muscle forces or proximal cephalometric measurements.
I fully appreciate that the evidence underpinning fixed appliance treatment is not high; yet there are trials of different brackets and functional appliances etc. I would also like to point out that we must remember that “conventional” orthodontists adopted self-ligation treatment, Invisalign and TADS with little critical analysis.
Is there a way forwards?
Putting these thoughts aside, I cannot help thinking that there might be something to this concept. We need to move forward and stop endlessly arguing the issues. We could do a study! At this early point, this could be a cohort study, in which a consecutive sample of patients could be enrolled; data would be collected at the start and end of treatment. All patients regardless of co-operation would be analysed and any failures would be recorded. Is this difficult to prepare? No this is straightforward, I could write the protocol in a couple of hours. Ethics would not be a problem.
So a challenge to those supporting these concepts is to get in touch with me. I will work with you to write the study, and we may be able to find funding (or this could be funded by the proponents of the methods). We will then remove all the uncertainty and argument. I will also give you the right of reply if you feel that I have misunderstood anything, and offer you a blog posting of about 1,000 words that I will publish in the next few weeks. It’s over to you….

Emeritus Professor of Orthodontics, University of Manchester, UK.
I was delighted reading this, Dr. O’Brien. So committed to disclosing the truth instead of just being prejudicious about… In fact, I think that this blog is a great gift to all of us! Thank you!
I’ve been looking into this form of treatment for about four years now. There does not appear to be any scientific studies to support this treatment modality. There are some case reports but not much else.
Dear Colleague,
rightly, the MFT with oral appliance needs more validation, too far away from scientific evidence. I feel, however, to remember with conviction that the Evidence Based Medicine is the integration of clinical expertise, patient values and (ALSO) the best evidence. There is not good literature on MFT and OA, but … the patient want MFT, we believe in MFT and we have very good results … we must have only the patience to convince the colleagues!
About this i would like to remember when, in the 1918, Alfred Rogers presented the MFT at the American Society of Orthodontics. In the 1950 presented again the same paper on MFT at the annual congress of the American Association of Orthodontics; the audience rose to their feet to applaud him because Rogers said “to this point I am afraid I have not been able to make a deep and lasting impression on many of our colleges. And this is why I present myself again to you to make an effort to show the worth of OMT, not just for the satisfaction that its intelligent application can bring the orthodontist but also for the many benefits it can bring a growing body “. Rogers waited over 30 years for the right tribute. Died in 1959.
Sir whats your opinion about MYOBRACE Applicance and Trainer by Dr Chris Farrell of sydney Australia.
Great start of a much needed discussion Kevin! Your statement ” I cannot help thinking that there might be something to this concept.” says it very well. For the past 30 years as an orthodontic specialist, I have practiced a philosophy of correcting malocclusions and facial disharmony by using my brand of functional facial orthopedics, typically followed by braces to get the best finished result I was able to. During that time, I developed a system to treat patients to achieve results that were consistent with what I termed “Nine Keys to Lower Facial Harmony” discussed in my book “Straight Talk about Crooked Teeth”. I laid out my Nine Keys in order of importance, which placed Fully Developed Maxilla as Key #1 and Unobstructed Nasal Breathing as Key #2. I am pleased to see that there is a lot more interest in Key #2 these days and even how it relates to Key #1. Even though one of the keys listed is Avoidance of Adverse Oral Habits as an etiologic factor, what the book was missing is the application of myofunctional treatment to correct these adverse habits at an early age. After the book was published in 2012, I was introduced to MRC appliances and have successfully used them for the past two years. With great patient cooperation amazing results are possible. To me this is a key missing link in orthodontics, to correct adverse oral habits while the patient is young, correcting and shaping positive future growth. Of course I always want to achieve the rest to the Nine Keys. I look forward to seeing the comments this blog will generate and certainly would like to take part and your proposed study. Kind regards, Kent
Your mention of a Fully Developed Maxilla as Key #1 resonated with me, given that mine is a full 6.8mm back. It’s been hurting my entire mouth, including molars, causing teeth decay, and scrapping my inner cheeks.
I’m in my mid-20s, and have been looking for a solution the past 3 years in different countries. Most solutions focus on children, is there anything for adults, especially for more severe cases like mine? (that doesn’t include more invasive methods like surgery, or extraction of 2 upper teeth for braces)
Thank you Dr Lauson, & Dr O’ Brien.
Dear Kent Lauson, I have just discovered myofunctional therapy and am wondering if you think it would be useful for my son who has a mild sleep apnoea due to enlarged tonsils (he is 8 now but has always had it). He also, over the last 3-4 years is experiencing neck pain and is starting sit with a hump and click his neck frequently. Nail biting has also made an appearance lately, however, bed wetting has stopped now. Would indeed tongue exercised be able to help him breath better and reduce the strain on his neck, back and nervous system. I have tried a number of things from osteopath, chiropractors, therapists but nothing with any result and I don’t want to drag him necessary through therapies if there isn’t a good reason now. Many many thanks in advance! Sanita
Hi… Fabulous reading… I’ve been very vocal in asking for evidence on the myofunctional appliances. Instructions: wear 1 hour a day, and at bedtime. How can you change (and if that even happens, maintain) the perioral musculature in a permanent way? I believe it has become a great source of revenue, rather than a great source of solutions. The research info they post on their website starts with E.H. Angle’s book from 1907…
Thank you for an interesting read Professor O’Brien. I’d like to bring the readers attention to another website with information about eruption guidance appliances and related research: http://www.lm-dental.com/products/orthodontic-appliances Particularly the sections “Research” and “Why treat early?” may be of interest to readers. We have tried to select high quality references when available but there is indeed room for more research. I hope you don’t consider my comment as exploiting your blog. If you do, I apologize!
Thanks, I have picked up on a really interesting unpublished trial (but advanced e publication) from your website. If I get time tomorrow I will post a blog on Monday about this paper. Best wishes: Kevin
Kevin, as a user of Biobloc, Myobrace, ALF, Myofunctional Therapy, and more, you might say I’ve drunk the Kool-aid on Myofunctional Orthodontics. And yet, my 25 preceding years as a specialist orthodontist, still has me questioning effectiveness and efficiency. I realize that Evidence Based Dentistry must rely on scientific evidence for one of it’s three pillars (the others being clinical experience and patient preferences and desires.) So I welcome all efforts at documentation and will be happy to participate. But there is one catch: Cooperation.
Your suggestion is to study efficacy regardless of cooperation. I suggest that that is a study in efficiency but not effectiveness. Since myofunctional orthodontics must address the function issues (as well as the form issues), we are necessarily tied to our patients’ commitment and compliance. (Perhaps this is the reason so many orthodontists are scared away from MFO.)
If you want to know if MFO really works, you must first look at cases that had GOOD cooperation. It’s the same with anything we TEACH our children. For instance,if we put 50 children through piano lessons and 25 of them quit, and 15 learned a little, and 7 still played as adults, and 3 became professional musicians, does that mean that piano lessons don’t work?
If we decided whether or not to send our children to school based on how willing they were to do their homework, what would we have? A generation of kids that don’t go to school!
If we let cooperation be the determining factor in whether or not we do MFO, what will we have? A generation of children that grow up with crooked teeth and need braces!
The problem with studying any holistic endeavor is that there always a range of results because there are so many variables that are at play. Reducing the variables to one for the sake of research often misses the bigger picture, unfortunately.
So, first look at the cases where cooperation was good to see if it works. Then join us in figuring out what the best way is to TEACH our kids the habits and patterns that will help them grow up straight and healthy. Then our job will be to skew the curve toward success.
Hi Barry, thanks for the comments. If we are to carry out a worthwhile health care investigation we need to include the data from all the patients who started treatment. Otherwise we will produce data that is biased towards the success. This would be similar to carrying out a drug trial and then excluding all the patients who did not improve or get better. I do not really go for the opinion that we cannot study this treatment. All we need to do is to identify a series of outcome measures and power the study sufficiently to analyse them. Unless we cannot identify an outcome measure and then we have a treatment that may be described as resulting in a change that no one can measure? Best wishes: Kevin
The problem with doing a study like this in a clinical setting is that it boxes the patient into a protocol that may not work for them. There is always an element of trial therapeutics. If I begin a treatment with Myobrace and I’m not getting cooperation, I am not going to keep going to complete the study. If I start with an ALF or Biobloc or myofunctional therapy or whatever, I have to do a n=1 study on the spot and adjust the therapeutics accordingly. It seems ridiculous to me to include patients that are not cooperating into a study of whether a therapeutic regimen works. Like using a jump rope, it works is you use it. It doesn’t if you leave it on the wall. Like school books, you don’t learn anything if you don’t crack the cover. If you can’t get a kid to wear the Myobrace (or whatever) you need to do a study of your staff protocols, not your appliances.
Thanks for the comment. However, we cannot run a study in which the patients who did not respond to treatment, for whatever, reason are excluded. This would simply provide biased results to the good and not give us a true picture of the effectiveness of the treatment.
Best wishes: Kevin
Great discussion, thank you. I agree with Dr. Rachael’s line of thinking. Essentially if a child/family are not compliant with a particular treatment, then the treatment is not actually occurring, so how can its effect be accurately measured? If the study is not measuring what is actually happening, does this render the study invalid because treatment is effectively not happening?
When thinking about removeable appliances here, my experience with many children who have been given off the shelf MYOBRACE find them difficult to tolerate and don’t wear them, hence the potential effects of using the device is not measurable. This is the same issue for all removeable devices and particular in very young children.
Compliance is a huge issue in clinical settings where the aims are to ‘change behaviour’ or engage cooperation and many factors come into play. This is a substantive and relevant topic in this particular discussion.
I think both sides might be looking at this too linearly, as an “either/ or” approach. And also reflects inherent problems with such scientific studies, often there might be insufficient qualifiers or points affecting data not fully considered.
I do think that excluding non-cooperative users is too one-sided. Yet when these non-cooperative users are included, it should take this non-cooperative factor into consideration, and there needs to be even further points on the reasons why.
For the example Sharon Moore gave, “(her) experience with many children who have been given off the shelf MYOBRACE find them difficult to tolerate and don’t wear them, hence the potential effects of using the device is not measurable. ”
Isn’t this very example a reflection of how that device may not be effective? Is the discomfort just an inherent part of all orthodontic procedures for this issue, or does it reflect an underlying reason why this device may not be that good?
Just my two cents.
I am late to the party here as usual, but to carry the comparison to a drug trial to its logical conclusion, it seems that it would not be a matter of excluding all patients who did not get better; only those who refused to take the medicine. Of course in a drug trial, it would be easier to detect the noncompliant, but to include them would seem to bias toward failure.
Thank you to Kevin for talking about a subject that is unknown to most parents. I am a mom of two children ages 8 and 4. I have had many jaw issues in my life. And unfortunately, my issues are difficult to fix without surgery. So I have done a lot of research in the last 6 years and came across the Alf and Biobloc. I feel like I am cursed and blessed at the same time. The first issue I have is the cost. And the second issue I have is compliance. How do the parents deal with compliance issues when they have spent so much money on these appliances which are not covered by insurance. I am literally driving myself crazy because I am torn between orthotropics and orthodontics. I have called more than 10 orthodontists to ask about biobloc or alf and no one knew what they were! So my daughter has seen two orthodontist, who specialize in jaw surgery such as cleft palate,both say her oral posture is great and that her jaws joints are healthy and she’s growing at a good rate. So I have been told to wait a year. Then I found an orthotropist who’s opinion was different. Biobloc for my daughter along with osteopathic work and Alf for my son who is 4! I also found a local dentist who knew what biobloc was and highly recommended it. I am feeling very frustrated and confused about all treatments! In all my efforts researching appliances, it seems that nobody really knows how to really properly guide the jaw growth and occlusion. Any advice on what to do as a parent would be greatly appreciated. I am feeling pretty lost.
Lisa
Hi Lisa, thanks for the message and I am sorry for the delay in getting back to you. You have asked some difficult questions. I think that the best way forwards is to ask the dentists you have seen what there training and experience has been. For example, the specialists would have done a three year full time training programme and be on the specialist list for orthodontists. You could also ask them the scientific evidence that they have used in their recommendations to you, Then you can base your decision on this information.
Prof Kevin:
A series of questions/comments;
1. What is the scientific definition of “myofunctional orthodontics”? I could not find one.
2. IMHO the word “orthotropics” is being used wrongly, according to its accepted, scientific definition. Consider the concepts of ‘thixotropy’, ‘anisotropy’ etc. and the use of the word “orthotropics” in a clinical sense loses its meaning. It may be that the word ‘orthotrophics’ (with a ‘p’) is what was actually intended to allude to some aspect of growth e.g. hypertrophy, dystrophy etc.
3. I studied Moss’ functional matrix hypothesis (which was first formulated by Van der Klauw) and communicated with him from England. In 2003, I attended his retirement symposium (Columbia University, New York) and we noted that the FMH was incomplete. I attempted to complete this work and it was published at the University of Michigan, Craniofacial Growth Series, 2004. The new concept, the Spatial Matrix Hypothesis, appears to withstand quite a few tests (e.g. malocclusion, TMJ dysfunction, obstructive sleep apnea, concussion etc) since it was first published.
4. It seems to me that most of the items you mention above come under the term “craniofacial epigenetics”, which includes “epigenetic orthodontics”. I defined these terms as follows; Craniofacial/epigenetic orthodontics use a person’s natural genes to correct and straighten the jaws, teeth, soft tissues and functional spaces, painlessly, using biomimetic appliances. The basis of this assertion is a person’s ‘genetic potential’, which has been mentioned historically but never defined. Here I define genetic potential as ‘producing the optimal outcome in the prevailing conditions, subject to a viable population(s) of stem cells’. Hope that helps –
Best wishes – Prof Dave Singh
Thanks for the useful comments. I used the terms that are currently used by those who developed these techniques. Maybe John or Mike Mew would like to answer these points? Best wishes: Kevin
Interested in your comments Kevin I am surprised that you did not agree that my identical twins paper was powerful. “All the conventionally treated faces looked worse after treatment and relapsed to an unacceptable extent unless permanently retained.” also “none of the orthotropic cases had relapsed ten years after treatment”. Best wishes John.
Thanks John, in my posting I said the level of published evidence was not high. This paper was a comparison of case series of only 6 patients in each group. The group were a mixture of prospectively and retrospectively analysed patients. 4 twins were treated by conventional orthodontics, 5 were treated by orthotropics and 4 were controls. This resulted in groups that are so small the results are subject to individual variation. As a result, this is a low level of evidence. I thought that this paper was interesting but the sample and group sizes were very small.
As I said we need to improve the evidence base by carrying out larger prospective studies and I am willing to help with this. Best wishes: Kevin
Have you ever heard of bayesian rationality? You can’t do a study with sufficient power to guarantee a specific cause and effect. There is enough evidence to rationally accept the position that traditional orthodontic treatment is masking the symptoms rather than fixing the root cause (i.e. the collapse of the maxilla); its foundations are built on a myopic and mechanistic theory that does not account for the affects between the organism and the environment.
Dear Kevin
As you mention in your blog, not much is new in orthodontics and when you have been in the orthodontic environment for some years you recognize most of the topics in the orthodontic congresses. Functional appliances have been used for many years and famous orthodontist have been having these thoughts since early in the 20 century. Viggo Andresen and Emil Herbst presented there early versions of the Activator and Scharnier in 1909. Their hypotheses was that with an orthodontic appliance try to normalize sagittal function. The problem is that we as orthodontists are very mechanical in our thinking and we always will like to rely on our biomechanics and our orthodontic appliances to do the work. What most, if not all orthodontist agrees on is that malfunction in many cases is the cause of malocclusions. With that in mind it is hardly rocket science to make the deduction that elimination of malfunction at an fairly early age would prevent or minimize the development of the malocclusion. We probably should have more cooperation with speech therapists specialized in oral myofunction. I am however, very well aware of that the research in this area also needs much more attention before you will be satisfied 🙂
Dear professor O´Brien
Thank you for remarkable blog and current issue of myofunctional orthodontics.
While reading your toughs and comments, especially last part; it felt like you were reviewing our research.
We made a study! A multicenter RCT study, in which a consecutive sample of patients ( n=105) were enrolled and randomly selected to use two different appliances with same protocol in order to correct large overjet. Data were collected at the start and end of treatment with 1-year post treatment follow up. Even qualitative part was done and cost-effectiveness is in progress. All patients regardless of co-operation have been analyzed and all failures have also been recorded. Intention to treat protocol was followed. Five years ago, at the WFO in Sydney, we presented preliminary results of this RCT on overjet correction comparing Andresen activator and prefabricated functional appliance. Today our study is in final stage of writing for publishing. Even this year at the WFO in London, final result will be presented as oral presentation.
More studies are needed and I would love to be a part of the collaboration team.
I hope to see you in London and continue discussion in this, to me, a very interesting subject.
Yours sincerely,
Emina Cirgic
In a supplementary material for the study by Papageorgiou et al. “What evidence exists for myofunctional therapy with prefabricated appliances? A systematic review with meta-analyses of randomised trials”. J Orthod. 2019 Dec;46(4):297-310 we read:
“Dr. E. Cirgic was contacted on July 25th, 2019 to request missing data (age, overbite changes, lip seal changes) and outcome data for either a common timepoint between groups or estimates adjusted for treatment duration (either as aggregate data or the trial’s dataset). No response has yet been received”
This is a very interesting discussion! Since, as a trained speech therapist, and having worked as an orofacial myologist for 40+ years and having been married to an orthodontist for 30+ years, I have to say that early intervention is a must. Not necessarily appliance therapy, but recognizing issues before they become muscle patterns that take years to correct. How many children do you see who have been in speech therapy for years, some 8-10 years, who carry those patterns into their adult life? I treat them weekly. One major issue that I find missing here is the mention of airway and the role that it plays in malocclusion. John Mew discusses it at length in all of his courses and describes himself as having grown a longer face than he might have liked. So, even if you do not intervene with orthodontic appliances, recognizing airway dysfunction and its potential for long-term dental and speech issues should be a responsibility of all of us by seeing patients early enough to assess and refer for intervention. (By the way, most speech therapists do not have expertise in assessment of these disorders. They simply do not get it in their training. That is why the field of Orofacial Myology was born and why I teach!)
Simply a plea from a parent’s perspective who has been struggling in vain to find the right thing to do for my son’s jaw, teeth, and mouth breathing problems – please proceed with the envisaged project in a spirit of full co-operation as quickly as you can; I lie awake at night in the meantime wondering which of the many orthodontists opinions I should accept from headgear, to myofunctional etc Parents need answers not ongoing uncertainty and disagreement about which approach offers long term stable results with minimum risk : PLEASE
thank you
Thanks for the comment. I am hoping to make more contacts and start the project soon. In the meantime, I would always recommend that you obtain an opinion from a specialist orthodontist for most treatment.
Specialist Orthodontists are not trained in Dento-Facial Orthodpaedics. They prefer to treat in the permanent dentition (see Sandra Coulson’s comment above), do not give consideration to airway problems in the young and do not work with Oral Myofunctional Therapists so why do you say, quote ” I would always recommend that you obtain an opinion from a Specialist Orthodontist for most treatment”?
Hi Kevin, I have just stumbled across your blog . I am a dentist based in Yorkshire and I have been providing myofunctional orthodontic (myobrace) therapy for about two years now. Cutting straight to the chase, it works beautifully but good patient compliance is essential. For this reason the majority of my time spent with each patient (and there is a lot of that) is spent reinforcing the principles of treatment and encouraging good compliance. I have changed the way I approach malocclusion accordingly and recommend children start treatment from the age of 6 upwards.
There aren’t many other examples in dentistry/medicine where a practitioner would spot a problem (in this case a malocclusion) wait for it to worsen and then treat it. Common sense alone would favour treating the complaint at source, which is my endeavour.
I think a good solid study is an excellent idea but I have to agree with previous correspondence that a double blind randomised control trial (gold standard) is going to be near impossible. Perhaps within the profession we need to agree on what good evidence actually is. We need to accept that some things are not easily testable in within the boundaries of our current system, and for these treatments we need to think outside the box a little. I can prove myobrace works, I have the cases all photographed from start to finish, I can’t provide scientific evidence though, the treatment is still valid nevertheless.
Anyway I’d love to have some further discussion with you on the matter
Regards
Dr S Bedford
Thanks for the comments. My feeling is that there is no real reason why we cannot do a trial into myofunctional orthodontics, we just need to be more open and be critical of our treatments. How many well documented cases have you and are the patients consented for research?
Dear Professor O’Brien
Thank you for this thread. As there is much discussion surrounding malocclusion with a natural or genetic origin, what are your thoughts on using an appliance such as ALF to correct a malocclusion created by poor orthodontistry? In my case, I had braces (train tracks) some 12 years ago which have left me with a malocclusion. Over this period, I have suffered from chronic facial pain, migraines, fatigue, nausea amongst a few other symptoms. Only now is it becoming apparent to me that it may be a result of my malocclusion owing to bad orthodontic work in the past. I am now having this malocclusion corrected with braces again (they’re on 4 weeks already) but have only discovered the concept of myofunctional appliances over the last few days. I am now worried that the braces may not suffice alone and am considering having them removed to pursue an ALF appliance first (which is a massive financial upheaval). Any advice is most gratefully received. Many thanks!
I’ll be happy to be a patient in the study. I was torn between Orthotropics and myobrace.. I am a class III tongue tied (soon to be released) and more than happy to be part of it.
I am a professor in France, age 54, with malocclusion and jaw issues due to 4 premolar extraction as a child. I am fascinated by this intellectual debate here—and the open-mindedness of all the participants–and am personally curious to know which will work better in my case of adult reverse orthodontics: functional appliances or braces.
If there are any studies in which you would like a VERY compliant and determined new “patient”, please do contact me. I live in Paris and could travel to anywhere in Europe or the New York area.
here is my email:
[email protected]
Many thanks for your posts. It is a pleasure to read professionals passionate about discovering the truths of new methods in a field which–from what I have learned–is far from being set in stone.
Hi
I really think you should come to the next myofunction Congress and see a wider and bigger picture, you never mentioned anything about airways and the effect on children and please look at Kevin Boyd and you will see the reason why early prevention is better than fix braces
Thank you
I am a medical doctor with a PhD. My two children were initially seen by several orthodentists who due to their severe class 3 malocclusions advised extraction of all 4 premolars and 4 wisdom teeth in both children. Then traintrack style braces and several jaw operations when older to reaslign the jaw, including the surgical exposing a completely occluded canine and putting a chain on it to pull it into the mouth. I was told that my children’s teeth would never improve without this dramatic course of treatment. Indeed I was also told that there was no way that the impacted canine would ever emerge naturally.
As a medic who was not taught about orthodentics at Med school, all this dramatic treatment did not seem to make sense. I asked 4 orthodentists whether there was a treatment which did not involve 8 teeth to be removed from each child but I was told there was no alternative. Fortunately my local dentist told me about the Mews in England. He said they had wacky ideas and I should see them.
Well I did and I am very glad I did as now two and a half years later they have no impacted teeth, they have had no teeth extractions, they now have no need for surgery of any form and have much more attractive faces and necks and their former breathing/sinus issues are gone. They are also doing better academically.
Actually what the Mews achieved was remarkable and makes total sense. By expanding the palate to a normal size there became room for the teeth (rather than traditional orthodentics which extracted teeth and caused bone shrinkage and the traintracks which constricted the maxilla then pulled it downwards- ie the wrong way). The Mews initially used bioblocs to expand the palate then myobrace to straighten the teeth.
Over these last few years, I have seen that all the kids who have had tooth extractions (hence jaw bone shrinkage) and train tracks appear to have had a significant visible deterioration in their facial attractiveness and function over time. It is really so sad and immoral what is happening and verging on child abuse as with age faces undergoing these ‘conventional’ treatments seem only to get less attractive and need permanent tooth retainers. Whereas by looking at the kids in the Mew’s waiting room and talking to their parents, I was staggered on their improvements in their teeth and facial beauty and function over time. They also need no permanent retainer as naturally positioned teeth are stable.
As an academic, I have been staggered by the hostility to this common sense of making the mouth a more normal better functioning part of the body by using orthotropics or myobrace. It does admittedly require persistance and a thick skin, as at many times- well a year or so- I got really really fed up with their moanings. That stage was really awful. However it is all really worth it now. My daughter is even mistaken for being a model, which makes her really happy.
Yes, a lot of orthodontics doesn’t make sense. The much-maligned orthotropists or whatever you want to call them at least posit a very straightforward aetiology of malocclusion that conforms with the fossil record and other basic evidence. They argue that most modern jaws are underdeveloped due to lifestyle and that we can fix a lot of issues by enlarging the maxilla. This basic premise informed my decisions about my daughter’s treatment. Her baby teeth fell out early and her adult teeth grew into a small mouth and were crowded. I had her palate expanded at 6 or 7, and all her teeth are now straight and she needs no further treatment, not even braces. By creating space, the teeth grew in straight, because that’s what they are genetically programmed to do. We are not encoded to have crowded teeth. My daughter’s experience is a far cry from the 8 years of painful intervention, including extractions, that I endured at the hands of an old-fashioned orthodontist with pretty bad long-term results. Most of O’Brien’s post just defend the status quo against what is a growing awareness that there is something not quite right with the orthodontic profession and its prescriptions. I actually think the simplicity of the orthotropist premise offends a lot of orthodontists and makes a lot of what they do redundant.
One more comment…I also combined the use of the biobloc and myobrace with a form of cranial manipulation. This manipulation loosens the cranial sutures allowing them to move into more optimal positions. I worked with a therapist with former experience in this form of cranial massage to create a way to speed up the movement of all the cranial bones to improve the jaw position, which then enabled the teeth to move into their correct position due to the increase in space. I did this as putting up with two teenagers moaning is hard work and I needed the final result as fast as possible.
Hi Paula, can you share details of where I can learn this cranial manipulation? My daughter started her upper jaw expansion at 10 , we are using a Schwarz style expander. I
Hope to find a Biobloc provider in Dublin to complete.. I’m also battling against time so
Wish to speed this
Up many thanks
Dear Professor O’Brien,
John Mew is influenced by Prof. Fränkel and Fränkel has described growth and its laws very precisely. He was primarily a developmental biologist and as such he spoke exclusively of spaces. The respiratory and oral functional space. So which development steps a child has to go through to develop regular function rooms. He has chronologically described in chronological growth events the necessary stages of development. The variables that interest orthodontists in growth and development are dynamic muscular and pneumatic forces (respiration). These are the cause of whether usable spaces develop. If the rooms are properly developed, the child has useful oral functions and also develops a regular chewing apparatus.
The tonic points, where the journey of development goes, are already set at about six months when the first teeth come. This should concern orthodontists, then they could draw the wrong conclusions from the wrong conclusions and would not methodically make such systemic mistakes. So orthopedics begins in infancy. Evidence-based medicine leaves little to be done if this understanding of growth and development proves to be correct, and there is much to be said for it.
Melvin L. Moss:
The “functional matrix” in its original version supports the general genome principle and explains exogenous influences on it. Fränkel found this too inaccurate in order to benefit from orthopedic benefits. His research and very precise observations made the errors of this theory visible and led to the evolutionary principle of indirect genetic control. The priorities are reversed. In his evaluated version (1997) Moss has corrected the “functional matrix” in the sense of Fränkel.
Neurobiological Foundations of Early Childhood Development (09.02.2018) Prof. Dr. med. Paul G. Layer)
An important conclusion from the perspective of developmental biology is the finding that genes alone can not produce an organism. Even with even finely tuned gene expression, the genetic information alone is not enough to – simply put – a whole organ, such as a brain, or even to create the whole person. Closely linked to this realization is the question of further mechanisms that guide the emergence of a functional structure. An initial answer to this is, for example, the consideration of neurogenesis in the context of embryogenesis. It shows that every single genetic action is always accompanied by spatial and temporal boundary conditions, which determine the further course of development significantly. The conclusion of these views can be summarized in the statement that effects of genes are always embedded in a time-space development corset, and only by interaction of genes with their given (molecular) “environment” a meaningful development process is made possible.
Dr. Paul G. Layer, Professor (i.R.) for Developmental Biology & Neurogenetics, Department of Biology, Darmstadt University of Technology.
This is why people turn to God for help. We don’t have answers. Desperate parents will do and pay anything for their child. Everyone has to pay bills and eat so their perspectives are skewed
I came to this post by googling the difference between biobloc and myobrace. Now I see that they should actually be combined. Kevin, thank you for your post. And everyone thank you for your comments. Having kids brings us a new challenge of becoming a medical specialist in various spheres. As we see that traditional methods and protocols can bring more harm than positive results. I am currently looking for specialists/clinics in Poland. If you have any recommendations I would be grateful.
It’s interesting that the author attributes the promotion of functional appliances primarily to John Mew. While Mew has certainly been influential, it’s important to remember that functional orthodontic devices have a long history and have been developed and utilized by many practitioners over the years. Figures like Frankel and others have made significant contributions to the field long before Mew’s concepts gained attention. It’s essential to recognize the broader historical context when discussing the development and impact of these treatment methods.