Pulsed electromagnetic field reduces orthodontic pain
Orthodontic pain is a major problem for our patients. This post is about a new technique that may reduce orthodontic pain.
Most orthodontist and dentists recommend analgesics to reduce orthodontic pain. Unfortunately, pain medication may have side effects or even reduce the rate of tooth movement. As a result, investigators have done research into non-pharmacological methods of pain relief, for example, vibration and low level laser light therapy. In this new study the investigators did a trial to evaluate the effectiveness of pulsed electromagnetic field (PEMF) on orthodontic pain. This new non-invasive therapy has been used to reduce pain in injured tissues. This team from several hospitals in Korea did this study using a small PEMF device. The AJO-DDO published this paper.
Jin-Gon Jung et al
Am J Orthod Dentofacial Orthop 2017;152:582-91 Doi: http://dx.doi.org/10.1016/j.ajodo.2017.04.022
They set out to answer this question;
“Did PEMF reduce orthodontic pain after they inserted initial arch wires”?
What did they do?
They did a single blind split-mouth 2 arm parallel randomised trial with a 1:1 allocation ratio. The PICO was
Participants: 33 female orthodontic patients aged 11-25 years having fixed appliance treatment to their upper teeth.
Intervention: PEMF in the form of a patch. The participants attached the patch to their cheeks (see picture). This generated an electromagnetic field of 27.12MHz. I think that this they applied this at 24, 48 and 72 hours after the first bond up.
Control: Placebo device. The device was not active.
Outcome: Pain recorded on a numerical rating scale from 1-10 (worst pain) over a period of 3 days. The investigators sent a survey form to the participants mobile phones 6 times over a 72 hour period. They collected the pain data at rest and while clenching their teeth.
They randomly allocated the active/placebo devices to each side of the participants mouth. The participants wore the devices for 7 hours on 3 consecutive nights. The patients were blinded to allocation.
What did they find?
Interestingly, they reported that pain was reduced for both clenching and resting states at 24, 48 and 72 hours after they placed initial arch wires. I have included a graphic from the paper. Hopefully, I have not broken copyright.
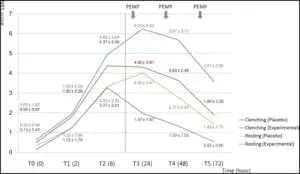
This shows that there is a reduction for both the placebo and the experimental groups with time.
What did I think?
Firstly, we need to consider that this was a small scale pilot study. This means that it only provides preliminary information and we need to be cautious. Nevertheless, the results are interesting and they certainly point to future studies.
We also need to remember that this was a split mouth study. As a result, we cannot be 100% certain that the intervention on one side of the mouth did not influence pain perception on the other side. For example, we can see from the graphic that the placebo reduced the level of pain. This may be a placebo effect or it maybe a true reduction because of the cross over.
My other concern is whether my patients would wear a patch on the outside of their face. It appears that the authors asked the patients to wear this device for 7 hours at night. Nevertheless, it was not clear if this was while they were asleep?
In summary, I thought that this was an interesting pilot study. Finally, it was also good to see a product tested before being introduced onto the market.

Emeritus Professor of Orthodontics, University of Manchester, UK.
I had done research into electromagnetic fields while doing my MSc in the late 1990s. Pulsed EM fields were (and still are) used to promote bone healing, though the evidence is, at best, equivocal. The opinion is that, while the EM field itself would have very little effect on cellular metabolism, there may be local heating, which would cause vasodilatation. This could be a possible explanation for the effects of the fields.
The comment ” pain medication may …… reduce the rate of tooth movement” is interesting. Why are we still using nociceptive techniques to move teeth? Pain medications such as NSAIDs (unlike aspirin) are thought to reduce pain without reducing the inflammatory process, which is used to move teeth – so is PEMF addressing the side effects of the protocol (such as pain) or the inflammatory process which is the underlying cause of the pain – I guess we need to read the entire Discussion –
NSAIDS (including ibuprofen) do reduce inflammation by inhibition of the enzyme cyclooxygenase (within the arachidonic acid pathway). However, over-the-counter doses of NSAIDs probably do not have a clinically significant effect on tooth movement. This may not be true for very high doses, but these doses are not appropriate for orthodontic induced discomfort.
WOW!!!! PEMF is really a powerful therapy to reduce annoying pain. I read a few articles on PEMF before it, but this content provides knowledge through experiment.
The graph used in this blog proves that PEMF is the best solution to get relief from pain.
NSAIDS (including ibuprofen) do reduce inflammation by inhibition of the enzyme cyclooxygenase (within the arachidonic acid pathway). However, over-the-counter doses of NSAIDs probably do not have a clinically significant effect on tooth movement. This may not be true for very high doses, but these doses are not appropriate for orthodontic induced discomfort.
Thanks for sharing this valuable information about pemf. It is important to know the effectiveness of pulsed electromagnetic field in orthodontic pain. From your blog, we get much important information on this topic.
Are you familiar with LIPUS?
Yes, there is an absence of evidence on its effects.