Does mode of breathing influence facial growth?
Does breathing influence facial growth?
This is my second post in the series on breathing and orthodontics and is concerned with the influence of breathing on facial growth. Many claims are made about this subject, but how closely have we looked at the evidence? I have had a good look at this, and this is my summary.
As I discussed last week, there is increasing interest in correcting children’s breathing with orthodontic treatment. But where is the evidence that supports this form of therapy? An excellent place to start is to consider whether breathing problems influence facial growth? Firstly, let’s look at some of the statements that are made;
“The airway breathing and orthodontics” Orthotown News, November 2015
Page and Mahoney state;
“Nasal obstruction, in particular, is a key villain and cause of abnormal growth and development of the face, jaws and dentition”. This is illustrated, in the magazine article, by a picture of the child with the classical “adenoid facies”.
Others are not sure definite, for example, Kate Vig in the American Journal of Orthodontics writes;
“The form function interaction that conveniently should explain the causal association between nasal obstruction and facial growth in children appears to be of a multifactorial nature”.
I have always found this to be a somewhat confusing area. It is also difficult to review because the literature is historic and challenging to interpret. I have decided to approach this by critically evaluating the papers that are frequently quoted by those who promote the theory that disordered breathing influences facial growth. So this selection of documents is from their publications and other reading lists that they produce.
 Primate experiments on mandibular growth direction
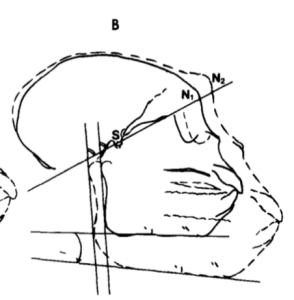
Primate experiments on mandibular growth directionIn the results section, they stated that there were significant differences between the two groups of monkeys. In brief, they found a significantly larger increase of the gonial angle and of the angle between sella-nasion and the lower border of the mandible in the experimental group. However, they did not present any data, and we have no indication of the magnitude of this difference. They illustrated this concept by showing some of the tracings. Overall, they concluded
“the steep mandibular plane angle and increased face height can be viewed as a result of an induced neuromuscular imbalance between the neck and facial muscles in the experimental monkeys”.
What did I think?
Firstly, I feel that I should show the respect that is due to the early orthodontic research workers and we need to consider that historical research papers do not always stand up to contemporary scrutiny concerning research methods. However, if we apply our current understanding of levels of evidence, we can only conclude that this paper is at the level of an interesting case report. Furthermore, I cannot help feeling that it is difficult to apply the findings to humans. This is because we do not really know if the results of these animal experiments are relevant to the facial growth of contemporary children. Also, the experimental monkeys had complete nasal occlusion, and this is unlikely to happen to children.
In summary, all that I can conclude is that this was an unusual case report and the results cannot really be applied to facial growth in children.
The other classic work is that carried out by Linder-Aronson and Woodside and I will revisit a post that I did some time ago.
Mandibular growth direction following adenoidectomy.
Linder-Aronson, S., Woodside, D. G., & Lundström, A. (1986).
American Journal of Orthodontics. doi:10.1016/0002-9416(86)90049-7
They carried out this study to evaluate the effect of adenoidectomy on a group of children with severe nasopharyngeal obstruction.
They selected a group of 81 Swedish children who had undergone adenoidectomies to relieve severely obstructed nasopharyngeal airways.
48 of these children changed from mouth to nose breathing, and this group formed their initial sample. They then followed 38 of these children for five years. This was their final sample.
All the children had the following records collected;
- Study models
- Lateral cephalometric and PA radiographs
- Airflow measurements recorded by rhinometry
At the following stages;
- T0 Before operation
- T1 1 year post-op
T3 5 years post-op
What did they find?
- Girls who had adenoidectomies had more horizontal growth than the girls in the control group. The difference in the position of gnathion was 11.5 degrees, and the 95% Ci was 2.25-20.75 (which is very wide)
- This difference was not found for the boys
- Growth direction was more variable for the adenoidectomy group than the control group
The mean airflow through the nose increased for the adenoidectomy group
They then revisited this data five years later and published another paper using a different cephalometric analysis, but this time they wanted to measure mandibular and maxillary growth.
They divided the sample up by gender and analysed these group differently. When they looked at maxillary growth in boys, the mean difference between the adenoidectomy and control group was 1.2mm (95% CI 0.00-2.4), there was no difference for the girls. Analysis of the data for the mandibular length revealed that for the boys the mean difference was 3.8 mm(95% CI 1.72-5.8) and for the girls, it was 2.5mm (0.79-4.2).
I think that these effect sizes are rather small and the 95% confidence intervals are large. This means that there is a large amount of uncertainty in the data and is a reflection of the small sample size.
They concluded;
“the establishment of nasal respiration with severe nasopharyngeal obstruction affects the amount of mandibular growth.”
This dataset was then revisited again when Mahoney et al., published a paper, 14 years later, using the same sample. This time they analysed the incisor and molar dento-alveolar heights and upper and lower anterior facial heights.
Mahoney et al.,
Aust Orthod J 2004; 20: 93–98
What did they find?
To be honest, I was not sure what they found because they did not present the data to show the differences between the adenoidectomy and control groups. I have looked closely at their results and calculated the difference between the control and the adenoidectomy group for Lower Anterior Facial Height. The difference between the two groups at the start of the study was 0.9mm (0.12-1.92) end of the observation period was 1.4mm (95% CI 0.03-2.8). I suggest that this is not a clinically significant difference and it has a very wide CI.
Nevertheless, they concluded that
“Before adenoidectomy mouth breathing children had significantly longer anterior facial heights than the control children and the strength of the difference lowered over time”.
The data does not support this conclusion.
What did I think?
I have looked carefully at these papers based on this classic sample of children, and there are several issues that we need to consider;
- This sample was derived from children with severe nasopharyngeal obstruction, and the findings are only valid for this severity of disordered breathing.
- The cephalometric differences that they detected were minimal and were not clinically significant.
- The sample had severe attrition bias
- They analysed the boys separately from girls, and I wonder if they had combined the two groups the differences would not be there?
- If you analyse multiple cephalometric variables several times, you will find something just by chance!
Summary
My first feeling on looking at these papers is one of disappointment that these papers did not really stand up to contemporary scrutiny.
I think that what we are currently seeing, from those who are promoting “curing disordered breathing” with orthodontics, is a classic non-critical selective quoting of historical data. This adds to the smoke and mirrors.
My only conclusion from these papers is that there is minimal evidence that mode of breathing has an effect on the craniofacial skeleton and facial growth.
I know that my opinion may be considered to be somewhat controversial. If you do not agree, have a good look at the papers and put your interpretation forward on the comments section of the blog. We can then have a chat about all this.

Emeritus Professor of Orthodontics, University of Manchester, UK.
Thanks Kevin. Interesting to see the historical papers on this subject. I have seen a benefit in a patient that had adenoidal surgery (not for orthodontic reasons) but she showed a clinical improvement in her AOB and vertical growth pattern. Purely anecdotal!!!
There is a very good paper about this in portuguese, (Rev. dent. press ortodon. ortopedi. facial;9(1):79-87, jan.-fev. 2004). I tried to find it in english but I could not. This paper states that if the patient presents tendency of long face pattern mode of breathing will influence it facial growth, otherwise if the patient presents tendecy of short face pattern the mode of breathing makes no statistically significance difference.
Hello Kevin,
About 30 years agoo, I was trained to become an orthodontist. My research was to mesure the dicferences in pressure on the dentition during mouth and during nose breathing. In my opinion not the way of breathing but the change in equilibrium should be investigated. I had to stop my researcb when it became clear that temparature differences caused bias.
Very nice!
I think your conclusions are correct.
Very weak evidence.
Thanks very much. I appreciate your blog!
Kevin, I don’t believe that your opinions or comments are controversial in the least.
What I do see however is that there is a lack of research into this issue – so I have 4 questions for you and your readers/contributors to consider:
1.Does the fact that the absence of contemporary research into this issue mean that the condition does not exist?
2. Is it not a fact that mouth breathing children and adults usually have low tongue posture?
3. Is there any doubt whatsoever that the tongue has a major influence over the growth and development of the teeth and jaws?
4. There are claims that “orthodontics ‘cures’ disordered breathing” (as quoted in the second paragraph of your Comments). If that relationship has any veracity, is the corollary not also maybe true – that ‘breathing could be a contributory factor in crooked teeth?
Finally – it is obvious from all of your posts and comments, as well as those of supporters and detractors alike, that the major issue here is ‘lack of contemporary research’, NOT lack of evidence of dysfunction. If there are bear tracks in the snow is it really necessary to follow them to prove the recent presence of a bear?
Thanks for the comments and I will answer your questions, as well as I can
1.Does the fact that the absence of contemporary research into this issue mean that the condition does not exist?
I think that the lack of good research into this condition does raise doubts whether growth is influenced by breathing.
2. Is it not a fact that mouth breathing children and adults usually have low tongue posture?
We do not know because the research does not confirm this theory
3. Is there any doubt whatsoever that the tongue has a major influence over the growth and development of the teeth and jaws?
There is no doubt that the tongue influences the position of the teeth, but I am not convinced about the jaws, the papers that I discussed in my blog post did not provide evidence that I would say is sufficiently strong to state this.
4. There are claims that “orthodontics ‘cures’ disordered breathing” (as quoted in the second paragraph of your Comments). If that relationship has any veracity, is the corollary not also maybe true – that ‘breathing could be a contributory factor in crooked teeth?
Again, there is no evidence that supports this suggestion. Have you any?
Finally- there may be a relationship, but the evidence is not there. If there are bear tracks and you want to catch the bear, it is probably a good idea to find out as much as you can about the bear, before you go on the bear hunt!
Wow! Thank you again for putting the time in to pull back the curtain on another controversial topic!
Kevin,
I agree… Not enough good evidence to back facial growth and breathing. This reminds me of my constant “encounters” with patients arriving at my orthodontic practice with miofunctional gadgets (Trainers), placed by GP’s and Pedodontists (and some orthodontists as well), claiming they are fixing breathing/tongue posture/swallowing/lips posture/lip activity/etc…., that would eventually rid the patient from needing fixed orthodontics, without mentioning the fact that their mandibles would grow significantly! And as much as I have looked for serious research on this appliance, I haven’t been able to land on any.
When I returned to Michigan in 1991, I inherited Peter Vig’s SNORT data and the accompanying longitudinal cephalograms. Armed with these materials, I advised a thesis by Kimberly Higgins.-Barber, 1992, that failed to find a relationship between breathing mode and subsequent facial growth. I was a naughty boy–I didn’t publish the data. I wasn’t a popular choice within the Department, so I had a lot of other things to think about.
Thanks Kevin for putting this controversial topic of the 20th century in perspective. When I published the AJODO article in 1998, which you kindly quoted, I was reviewing Nasal obstruction and Facial growth from the strength of evidence for clinical assumptions. As Lysle mentions much of the data was from Peter Vig’s expertise on the subject. While an evidence-based approach was beginning to gain traction I was fortunate to have been at the University of Michigan when David Sackett was involved in the symposia. He made an impact on my confusion about what to believe about facial growth and breathing. The result was my first and worst attempt at a systematic review which raised more questions than it answered. This abiding interest of Orthodontists in the airway seems to have now morphed into sleep disordered breathing with more severe medical consequences and one in which orthodontists may use “functional” appliances with the objective of increasing the oropharyngeal airway instead of growing young mandibles.
Katherine, It’s such an honor to have you here… Can you tell us your take on Harvold’s work? There must have been something that intrigued us enough to follow this line of research. I know that each of the monkeys found a different way to compensate for nasal obstruction and the consequences varied widely. Did that cause some confusion?
Barry – It is a while since I read the Egil Harvold & Karin Vargervik’s paper on complete nasal obstruction in non-human primates (monkeys). After 2 years the monkeys developed an increase in vertical facial height, an oral airway and open bite. This was considered irrefutable evidence that nasal obstruction directly affects facial growth. Harvold was able to completely obstruct the nasal airway in his experimental studies – to survive the animals had to adopt an oral mode of respiration. This rarely occurs in humans who typically have an oro-nasal airway. With individual biological variation facial growth will vary in its expression and resulting response . The amount of nasal obstruction tolerated, before supplementing airflow with oral respiration, is multifactorial and difficult to measure. This 20th century controversy has continued into the 21st century but the focus has changed to sleep disordered breathing and its treatment and consequences .
I just found this article in the BMJ: http://bmjopen.bmj.com/content/5/9/e009027.full
I agree the evidence is lacking that it should be researched more. This study is a great start. I wander if orthodontics and tooth extractions might cause a similar effect to SBD in young people? What do you think Kevin?
I have followed the debate with interest and so I have looked at the study cited above (Ali et al. The influence of snoring, mouth breathing and apnoea on facial morphology in late childhood: a three-dimensional study. BMJ Open 2015;5:e009027 doi:10.1136/bmjopen-2015-009027).
The researchers examined data from a large longitudinal cohort study and did indeed report differences in facial measurements between the children with and without self-reported SDB throughout early childhood. Young people with self-reported SDB showed:
An increased face height of 0.3 mm (95% CI −0.52 to −0.05);
A decrease in mandibular prominence of 0.9° (95% CI −1.30 to −0.42)
A decrease in nose prominence of 0.12 mm (95% CI 0.00 to 0.24)
A decrease in nose width of 0.72 mm (95% CI −0.10 to −0.25).
Hmmm……
Kevin:
I like your response when you say “I think that the lack of good research into this condition does raise doubts whether growth is influenced by breathing.” Excellent.
To me this means we might be asking the ‘wrong’ research question(s). A better research question might be “Does mode of feeding influence craniofacial growth? And then, “Do subsequent craniofacial growth changes influence breathing”. These research questions are based on the Spatial Matrix Hypothesis, which took Moss’ functional matrix into account at the outset. One of the things about Dr Moss’ hypothesis was that it did not include the teeth. When I added teeth into the equation, I was better able to formulate the why and how a little better (IMHO) to predict aberrant craniofacial conditions, such as; malocclusions, TMJ dysfunction and sleep/breathing disorders. Indeed, once the etiology of these conditions is elucidated, then corrective clinical protocols can be devised. I could go into details but then this message becomes really long, but the take message is this: All modern human babies are obligate nasal breathers at birth, when they change from placental oxygenation to external respiration. One of the key molecules in this switch is, of course, NO – which is produced in the sinuses. The other crucial condition is that all modern human babies are still ‘mammals’, and mammals “exclusively” suckle/breastfeed/nurse their offspring or the offspring die. Hence, changes in early feeding behavior/early child rearing practices might influence craniofacial growth by changing the spatial matrices, such as the position of the tongue, position of teeth thru changes in the shape/size of the bony architecture, following epigenetic mechanisms, which yield a host of craniofacial conditions, including deformational plagiocephaly, nasal obstruction/mouth-breathing, adenoid facies inter alia.
The mouth breathing long faced theory is very seductive . Intuitively seems to make sense . So many great theories and opinions with so little conclusive research . The profession is still in its infancy . Great subject to bring up . We all benefit reading this great blog . Keep them coming Kevin . Love it .
While you guys debate the small points and hide behind the lack of evidence, I will continue to address both form and function in young children to help them grow as healthy as they can.
We could have the same discussion as above about the evidence of diets and weight loss, and yet I think we’d all agree it is prudent to eat healthy, real food.
We could have the same discussion about exercise and heart disease, and yet we’d all agree that getting out for a walk at the very least is a good habit to have.
We could have the same discussion about the relationship of sleep to IQ, cognitive function and car accidents, and yet we’d all agree that getting a solid 8 is a good thing do.
Even a Philadelphia lawyer in the 1870’s could see that mouthbreathing and snoring were not healthy signs, as did the native Americans that George Catlin regularly visited (His book “Shut your mouth and save your life” was promoted by Angle in 1925, btw)
So why are we having such trouble understanding that breathing properly is a good thing?
Can it be that the nose was designed for breathing? Do we need research for that?
There are so many ways in which human civilization has created compensations to deal with the way WE have changed our world since we left the savannah. (Including braces). Read Lieberman about the way our bodies have had to adapt to changing circumstances. The anthropologic evidence suggests that our faces are not growing the way our genetics – which has not changed substantially for the past 200,000 years – had programmed them to grow. The changes to our faces are relatively recent and rapid. There is very little malocclusion until recently (Let this be your next topic, Kevin).
So all this talk and debate about the evidence only serves one purpose: it allows us to continue to shed responsibility for these greater health concerns in our children and only pay attention to their teeth AS IF they are the real problem. The teeth are NOT the problem. They are merely a symptom. Like clogged arteries are a symptom. Like hyperglycemia is a symptom. Like swollen tonsils and adenoids are a symptom. Like open mouth posture, mouth breathing, swallowing using the facial muscles, and forward head posture are symptoms.
You may continue to argue about whether the symptoms mean anything while you continue treating the symptoms (with mechanics, surgery and potions). In the meantime, let’s have some of us try to deal with the WHY, and help these children get better. Snake oil, anybody?
Thank you for your comments Barry!
Maybe a more cautious approach is for us to simply screen for potential breathing problems and if we think there is potential for a significant breathing problem then refer (or participate as part of a multidisciplinary team) to the paediatric ENT (and maybe other health specialists) for appropriate diagnosis and management. We are not actually trained or likely not even licensed to diagnose and treat breathing problems. If this referral and posterior management does actually produce significant overall health benefits we should be pleased with our actions.
As for the influence or lack of it of changing of mode of breathing on craniofacial growth there is lack of solid evidence either way. Therefore any hypothesis is possible until proven otherwise. My humble opinion is that the key lays in how we do communicate this uncertainty to our patients so that they can make an informed decision. The way we communicate those concepts can significantly bias the patient’s treatment decision. Are we doing a fair and professional job in this regard based on how little we know?
We don’t treat heart disease either, Carlos, but we do take blood pressure as part of our exams. We don’t treat cancer, but we do screen for lumps and bumps in the face. You don’t need to be a pulmonologist to look at the following maladies in breathing:
1) Is the nose obstructed or congested in any way chronically?
2) Are the lips apart at rest?
3) Does the tongue rest on the palate and stay there during swallowing?
4) Are the chest or shoulders moving during breathing instead of the diaphragm.
5) Is the child’s rate of breathing greater than 16 breaths per minute?
6) Is the child holding their head in front of their shoulders (to keep their airway open)?
7) Does the child have any sleep issues like restlessness, enuresis, frequentl awakenings, or snoring?
Do we really need to be an MD to ask these questions? If your child was in an orthodontist’s chair and these questions WEREN’T asked and these problems missed, would you be happy?
Or maybe we shouldn’t take blood pressure or do cancer screenings because orthodontics doesn’t cause hypertension or cancer….Oh, wait….Did you know that David Gozal, president of the American Thoracic Society is showing research (RESEARCH, Kevin) that shows that obstructive sleep apnea CAUSES obesity, is associated with increased rates of growth with cancer, and spikes blood pressure at night enough to kill (We just lost one of our Supreme Court Justices because he forgot to put his CPAP on?)
And we’re still arguing about whether or not to look at the airway and breathing?
Sir, I strongly believe mode of breathing affects craniofacial growth. Not only this but the other symptom of UARS in children eg. ADHD. My own niece had suffered difficult breathing, snoring at night, reduced oxygen saturation while snoring and difficulty in learning long spellings in class. Advancing the mandible cured her ADHD to some extent but irregular treatment could not stimulate favorable growth.
Similarly I have observed long faces and difficult breathing in functional retrusion of mandible.